

Classifying late-onset dementia with MRI: is arteriosclerotic brain degeneration the most common cause of Alzheimer's syndrome?
- PMID: 18488889
- PMCID: PMC2544365
- DOI: 10.2147/cia.s2537
Classifying late-onset dementia with MRI: is arteriosclerotic brain degeneration the most common cause of Alzheimer's syndrome?
Abstract
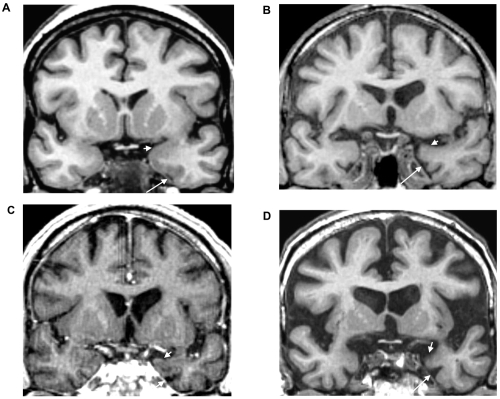
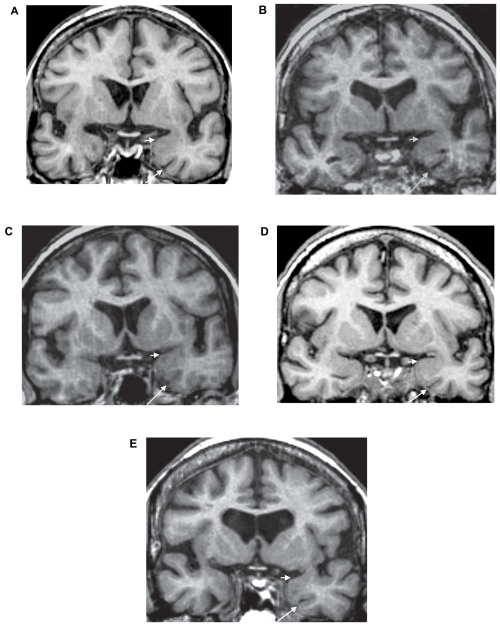
Our aim was to use early magnetic resonance imaging (MRI) to investigate the causes of cognitive decline in elderly people with mild cognitive impairment (MCI). Baseline structural and flow quantification MR sequences, and clinical and neuropsychological follow-up for at least two years, were performed on 62 elderly subjects with MCI. Of these subjects, 17 progressed to dementia, and 15 of these progressed to dementia of the Alzheimer type (DAT). Conversion to clinically diagnosed DAT was related to six distinct MR profiles, including one profile suggesting severe AD (20% of these converters) and five profiles suggesting severe cerebrovascular dysfunction. Two profiles suggested arteriosclerotic brain degeneration, one profile suggested severe venous windkessel dysfunction, and two suggested marked cerebral hypoperfusion associated with very low craniospinal compliance or marked brain atrophy. As compared with vascular MR type converters, AD MR type converters showed high executive and mobility predementia performances. Severe whole anteromesial temporal atrophy and predominantly left brain atrophy on visual MR analysis was only observed in AD MR type converters. In conclusion, these observations enhance the pathogenic complexity of the Alzheimer syndrome, and suggest that the role of arteriosclerotic brain degeneration in late life dementia is underestimated.
Conflict of interest statement
Figures
Similar articles
-
MRI of the 'Alzheimer syndrome'.J Neuroradiol. 2007 Oct;34(4):220-7. doi: 10.1016/j.neurad.2007.07.002. Epub 2007 Aug 24. J Neuroradiol. 2007. PMID: 17719631 Review.
-
Alzheimer's disease in late-life dementia: a minor toxic consequence of devastating cerebrovascular dysfunction.Med Hypotheses. 2008;70(4):866-75. doi: 10.1016/j.mehy.2007.07.027. Epub 2007 Sep 6. Med Hypotheses. 2008. PMID: 17825499
-
Assessing cerebrovascular contribution to late dementia of the Alzheimer's type: the role of combined hemodynamic and structural MR analysis.J Neurol Sci. 2009 Aug 15;283(1-2):44-8. doi: 10.1016/j.jns.2009.02.325. Epub 2009 Mar 5. J Neurol Sci. 2009. PMID: 19268312
-
MRI abnormalities associated with mild cognitive impairments of vascular (VMCI) versus neurodegenerative (NMCI) types prodromal for vascular and Alzheimer's dementias.Curr Alzheimer Res. 2005 Dec;2(5):579-85. doi: 10.2174/156720505774932241. Curr Alzheimer Res. 2005. PMID: 16375661
-
Intracranial MR dynamics in clinically diagnosed Alzheimer's disease: the emerging concept of "pulse wave encephalopathy".Curr Alzheimer Res. 2009 Dec;6(6):488-502. doi: 10.2174/156720509790147124. Curr Alzheimer Res. 2009. PMID: 19747161 Review.
Cited by
-
Changes in intracranial venous blood flow and pulsatility in Alzheimer's disease: A 4D flow MRI study.J Cereb Blood Flow Metab. 2017 Jun;37(6):2149-2158. doi: 10.1177/0271678X16661340. Epub 2016 Jan 1. J Cereb Blood Flow Metab. 2017. PMID: 27492950 Free PMC article.
-
Ratio between carotid artery stiffness and blood flow - a new ultrasound index of ischemic leukoaraiosis.Clin Interv Aging. 2016 Jan 25;11:65-71. doi: 10.2147/CIA.S94163. eCollection 2016. Clin Interv Aging. 2016. PMID: 26869775 Free PMC article.
-
Intracranial atherosclerosis as a contributing factor to Alzheimer's disease dementia.Alzheimers Dement. 2011 Jul;7(4):436-44. doi: 10.1016/j.jalz.2010.08.228. Epub 2011 Mar 9. Alzheimers Dement. 2011. PMID: 21388893 Free PMC article.
-
Structural magnetic resonance imaging for the early diagnosis of dementia due to Alzheimer's disease in people with mild cognitive impairment.Cochrane Database Syst Rev. 2020 Mar 2;3(3):CD009628. doi: 10.1002/14651858.CD009628.pub2. Cochrane Database Syst Rev. 2020. PMID: 32119112 Free PMC article.
-
The Impact of Aging on the Association Between Aortic Stiffness and Cerebral Pulsatility Index.Front Cardiovasc Med. 2022 Feb 9;9:821151. doi: 10.3389/fcvm.2022.821151. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35224051 Free PMC article.
References
-
- Bateman GA, Levi CR, Schofield P, et al. The pathophysiology of the aqueduct stroke volume in normal pressure hydrocephalus: can co-morbidity with other forms of dementia be excluded? Neuroradiol. 2005;47:741–8. - PubMed
-
- Bateman GA, Levi CR, Schofield P, et al. Quantitative measurements of cerebral haemodynamics in early vascular dementia and Alzheimer’s disease. J ClinNeurosci. 2006;13:563–8. - PubMed
-
- Bateman GA, Loiselle AM. Can MR measurement of intracranial hydrodynamics and compliance differentiate which patient with idiopathic normal pressure hydrocephalus will improve following shunt insertion? Acta Neurochir (Wien) 2007;149:455–62. - PubMed
-
- Baumbach GL. Effects of increased pulse pressure on cerebral arterioles. Hypertension. 1996;27:159–67. - PubMed
-
- Bell-McGinty S, Lopez OL, Cidis-Meltzer C, et al. Differential cortical atrophy in subgroups of mild cognitive impairment. Arch Neurol. 2005;62:1393–97. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
