

Implications and management of pancreatic fistulas following pancreaticoduodenectomy: the Massachusetts General Hospital experience
- PMID: 18490557
- PMCID: PMC3806102
- DOI: 10.1001/archsurg.143.5.476
Implications and management of pancreatic fistulas following pancreaticoduodenectomy: the Massachusetts General Hospital experience
Abstract
Objective: To describe the management and impact of pancreatic fistulas in a high-volume center.
Design: Retrospective case series.
Setting: Tertiary academic center.
Patients: Five hundred eighty-one consecutive patients who underwent pancreaticoduodenectomy from January 2001 through June 2006.
Main outcome measures: Development of a pancreatic fistula (defined as > 30 mL of amylase-rich fluid from drains on or after postoperative day 7, or discharge with surgical drains in place, regardless of amount); the need for additional interventions or total parenteral nutrition; other morbidity; and mortality.
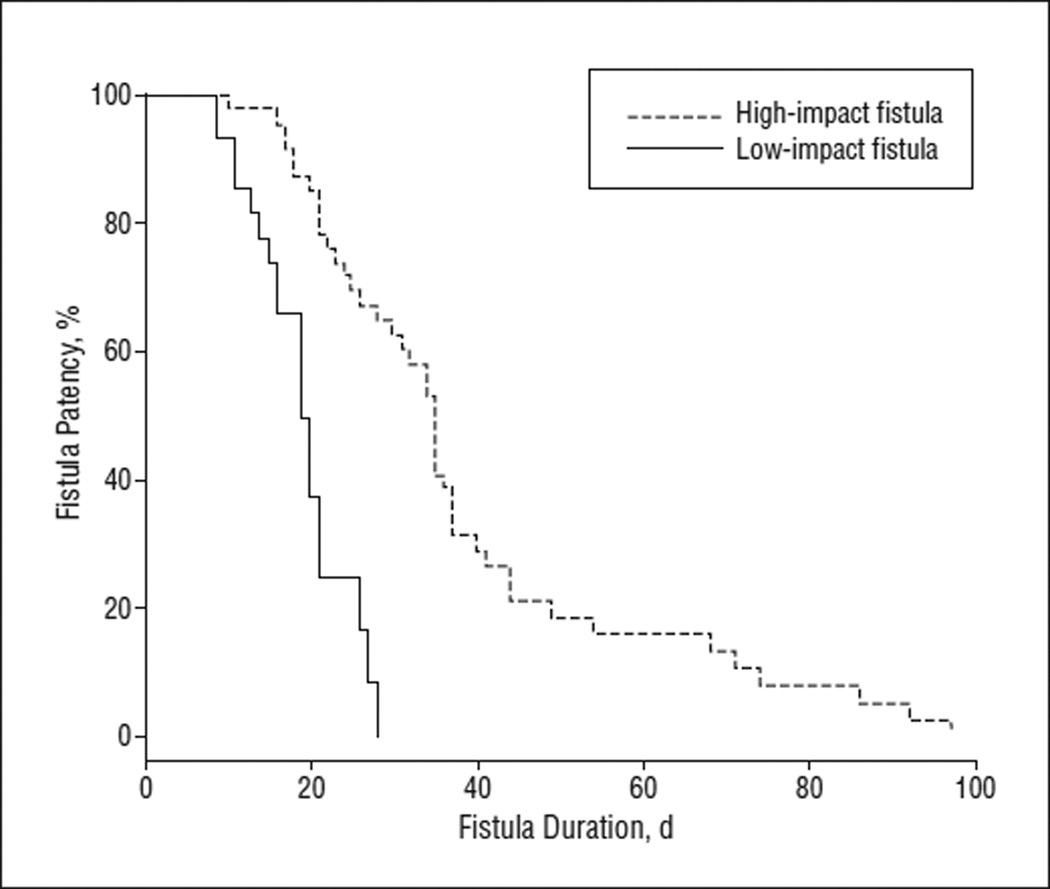
Results: Seventy-five patients (12.9%) developed a pancreatic fistula. Fistulas were managed with gradual withdrawal of surgical drains. This allowed for patient discharge and eventual closure at a mean of 18 days in 38.7% of cases; these were classified as low-impact fistulas. The remaining 46 patients (61.3%) had an associated abscess, required percutaneous drainage or total parenteral nutrition, or developed bleeding; these were classified as high-impact fistulas and closed a mean of 35 days after surgery. Standard 30-day in-hospital mortality was 1.9% for all pancreaticoduodenectomies and 6.7% for those who developed a pancreatic fistula. The overall fistula-related mortality was 9.3% (7 patients), all but 1 of which was related to major hemorrhage.
Conclusions: More than one-third of pancreatic fistulas are clinically insignificant (low impact). The remaining 60% of fistulas have a high clinical impact and nearly an 8-fold increase in overall mortality.
Figures
Comment in
-
Clinically significant pancreatic fistulas.Arch Surg. 2008 Nov;143(11):1132; author reply 1132-3. doi: 10.1001/archsurg.143.11.1132-a. Arch Surg. 2008. PMID: 19015476 No abstract available.
References
-
- Bassi C, Dervenis C, Butturini G, et al. Post-operative pancreatic fistula: an international study group (ISGPF) definition. Surgery. 2005;138(1):8–13. - PubMed
-
- Kazanjian KK, Hines OJ, Eibl G, Reber HA. Management of pancreatic fistulas after pancreaticoduodenectomy: results in 437 consecutive patients. Arch Surg. 2005;140(9):849–855. - PubMed
-
- Aranha GV, Aaron JM, Shoup M, Pickleman J. Current management of pancreatic fistula after pancreaticoduodenectomy. Surgery. 2006;140(4):561–569. - PubMed
-
- Choi SH, Moon HJ, Heo JS, Joh JW, Kim YI. Delayed hemorrhage after pancreaticoduodenectomy. J Am Coll Surg. 2004;199(2):186–191. - PubMed
-
- Muscari F, Suc B, Kirzin S, et al. French Associations for Surgical Research. Risk factors for mortality and intra-abdominal complications after pancreaticoduodenectomy: multivariate analysis in 300 patients. Surgery. 2006;139(5):591–598. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
