

A lack of amyloid beta plaques despite persistent accumulation of amyloid beta in axons of long-term survivors of traumatic brain injury
- PMID: 18492093
- PMCID: PMC3014260
- DOI: 10.1111/j.1750-3639.2008.00176.x
A lack of amyloid beta plaques despite persistent accumulation of amyloid beta in axons of long-term survivors of traumatic brain injury
Abstract
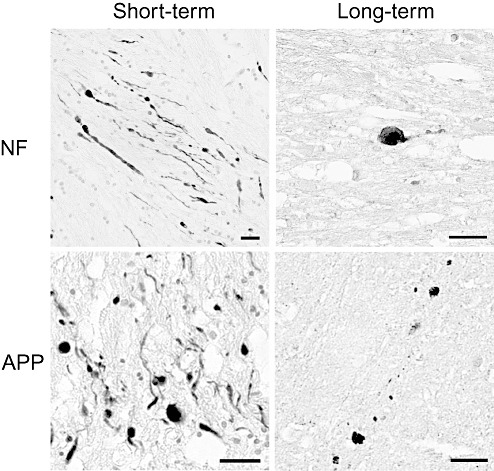
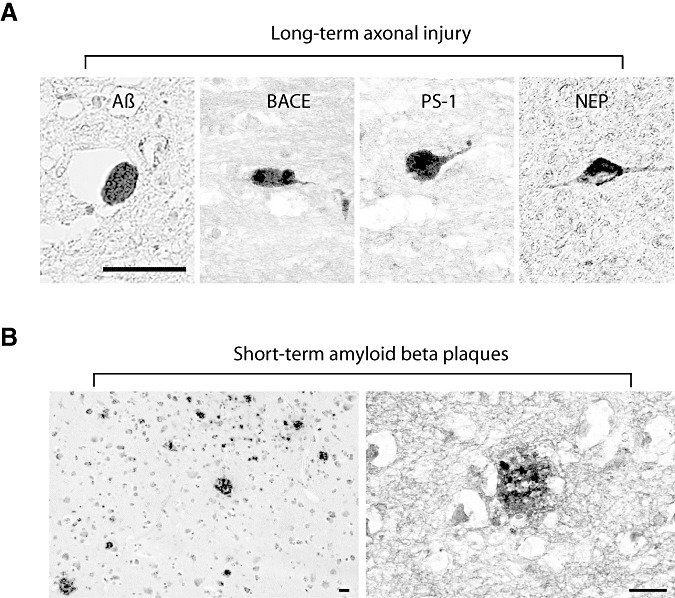
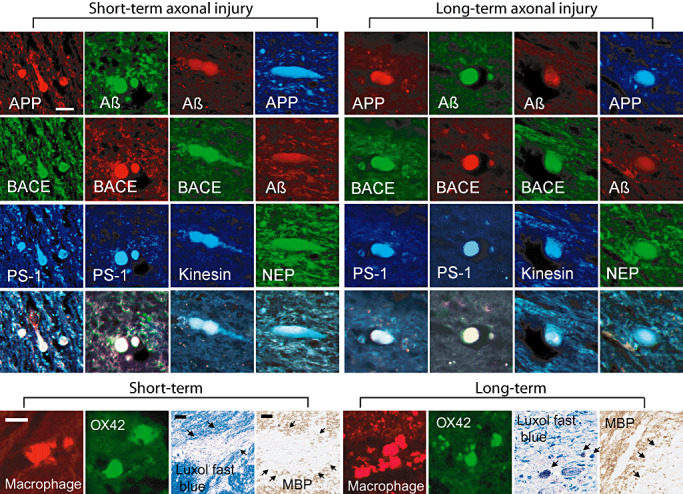
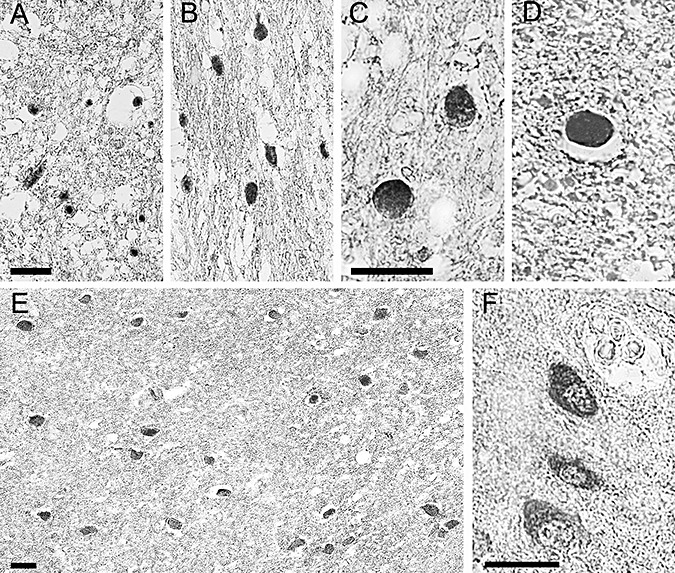
Traumatic brain injury (TBI) is a risk factor for developing Alzheimer's disease (AD). Additionally, TBI induces AD-like amyloid beta (Abeta) plaque pathology within days of injury potentially resulting from massive accumulation of amyloid precursor protein (APP) in damaged axons. Here, progression of Abeta accumulation was examined using brain tissue from 23 cases with post-TBI survival of up to 3 years. Even years after injury, widespread axonal pathology was consistently observed and was accompanied by intra-axonal co-accumulations of APP with its cleavage enzymes, beta-site APP cleaving enzyme and presenilin-1 and their product, Abeta. However, in marked contrast to the plaque pathology noted in short-term cases post TBI, virtually no Abeta plaques were found in long-term survivors. A potential mechanism for Abeta plaque regression was suggested by the post-injury accumulation of an Abeta degrading enzyme, neprilysin. These findings fail to support the premise that progressive plaque pathology after TBI ultimately results in AD.
Figures
References
-
- Adams JH, Doyle D, Ford I, Gennarelli TA, Graham DI, McLellan DR (1989) Diffuse axonal injury in head injury: definition, diagnosis and grading. Histopathology 15:49–59. - PubMed
-
- Adams JH, Graham DI (1976) The relationship between ventricular fluid pressure and the neuropathology of raised intracranial pressure. Neuropathol Appl Neurobiol 2:323–332.
-
- Adams JH, Graham DI, Jennett B (2000) The neuropathology of the vegetative state after an acute brain insult. Brain 123:1327–1338. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
