

Cigarette smoking associates with body weight and muscle mass of patients with rheumatoid arthritis: a cross-sectional, observational study
- PMID: 18492239
- PMCID: PMC2483449
- DOI: 10.1186/ar2429
Cigarette smoking associates with body weight and muscle mass of patients with rheumatoid arthritis: a cross-sectional, observational study
Abstract
Introduction: Rheumatoid arthritis (RA) is associated with altered metabolism leading to muscle wasting. In the general population, cigarette smoking is known to affect body composition by reducing fat and inhibiting muscle synthesis. Even though smoking has been implicated in the pathophysiology and progression of RA, its possible effects on body composition of such patients have not been studied. This cross-sectional study aimed to identify potential associations of smoking with body weight and composition of RA patients.
Methods: A total of 392 patients (290 females) with RA were assessed for body mass index (BMI), body fat (BF), fat-free mass (FFM), and waist circumference. Erythrocyte sedimentation rate, C-reactive protein, Disease Activity Score-28, and Health Assessment Questionnaire score were used to assess disease activity and severity. Smoking habit (current smoker, ex-smoker, or never-smoker) and intensity (pack-years) were also noted.
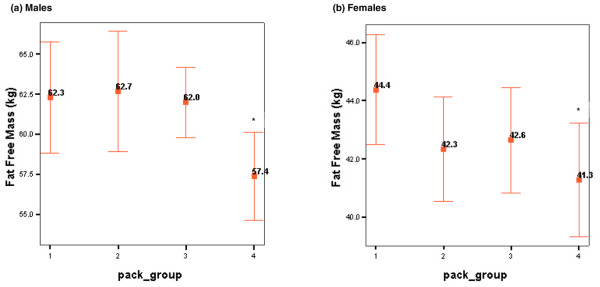
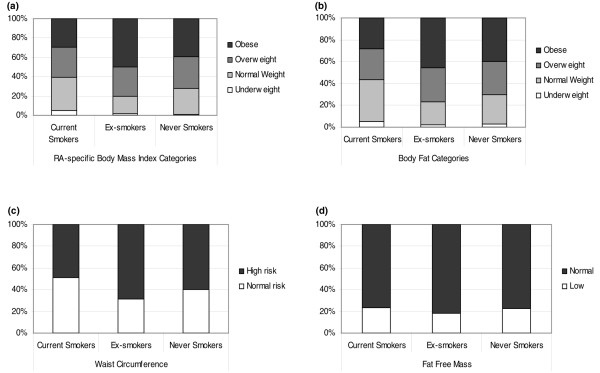
Results: Current smokers had a significantly lower BMI compared with ex-smokers (mean difference: male -2.6, 95% confidence interval [CI]: -3.5 to -1.7; female: -2.6, 95% CI: -4.8 to -0.5) and never-smokers (mean difference: male -1.8, 95% CI: -3 to -0.6; female: -1.4, 95% CI: -2.4 to -0.4). Similarly, the BF of current smokers was lower compared with that of ex-smokers (mean difference: male: -4.3, 95% CI: -7.5 to -1.2; female: -3.4, 95% CI: -6.4 to -0.4) and never-smokers (mean difference: male: -3.3, 95% CI: -6.3 to -0.4; female: -2.1, 95% CI: -4 to -0.2). FFM did not differ between groups. Finally, current smokers had a significantly smaller waist circumference compared with ex-smokers only (mean difference: male: -6.2, 95% CI: -10.4 to -1.9; female: -7.8, 95% CI: -13.5 to -2.1). Following adjustments for age, disease duration, and HAQ score, smoking remained a significant predictor for BMI (P < 0.001), BF (P < 0.05), and waist circumference (P < 0.05). Pack-years were inversely correlated with BF (r = -0.46; P < 0.001), and heavy smokers exhibited a significantly lower FFM (P < 0.05) compared with all other participants.
Conclusion: Within the limitations of a cross-sectional study, it appears that cigarette smoking associates with reduced BMI and BF in patients with RA and heavy smoking associates with lower muscle mass. Smoking cessation appears to associate with increased BMI, BF, and waist circumference in these patients. These results should be confirmed in prospective studies. Given the numerous adverse effects of smoking on general health and RA, patients should be actively advised against it. However, smoking cessation regimes in RA may need to include more general lifestyle counselling, particularly about weight control.
Figures
References
-
- Metsios GS, Stavropoulos-Kalinoglou A, Koutedakis Y, Kitas GD. Rheumatoid cachexia: causes, significance and possible interventions. Hospital Chronicles. 2006;1:20–26.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
