

Randomized trial comparing daily interruption of sedation and nursing-implemented sedation algorithm in medical intensive care unit patients
- PMID: 18492267
- PMCID: PMC2481461
- DOI: 10.1186/cc6908
Randomized trial comparing daily interruption of sedation and nursing-implemented sedation algorithm in medical intensive care unit patients
Abstract
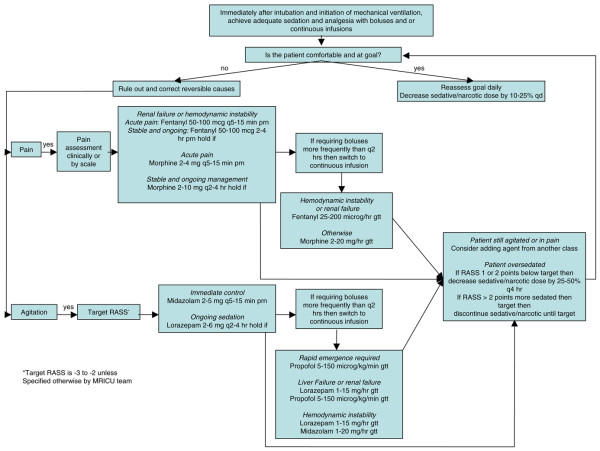
Introduction: Daily interruption of sedation (DIS) and sedation algorithms (SAs) have been shown to decrease mechanical ventilation (MV) duration. We conducted a randomized study comparing these strategies.
Methods: Mechanically ventilated adults 18 years old or older in the medical intensive care unit (ICU) were randomly assigned to DIS or SA. Exclusion criteria were severe neurocognitive dysfunction, administration of neuromuscular blockers, and tracheostomy. Study endpoints were total MV duration and 28-day ventilator-free survival.
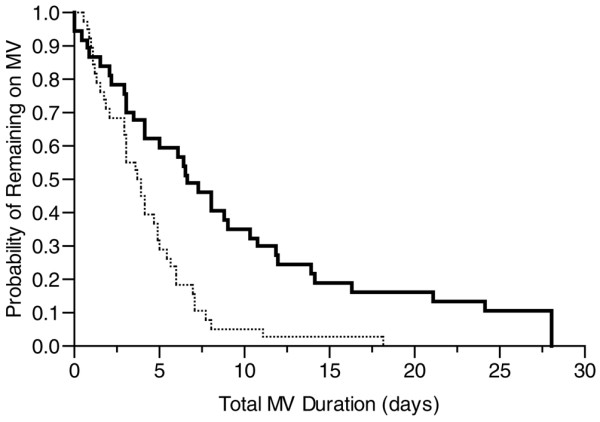
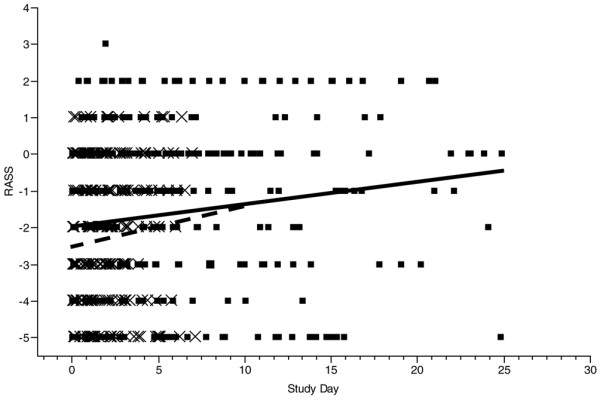
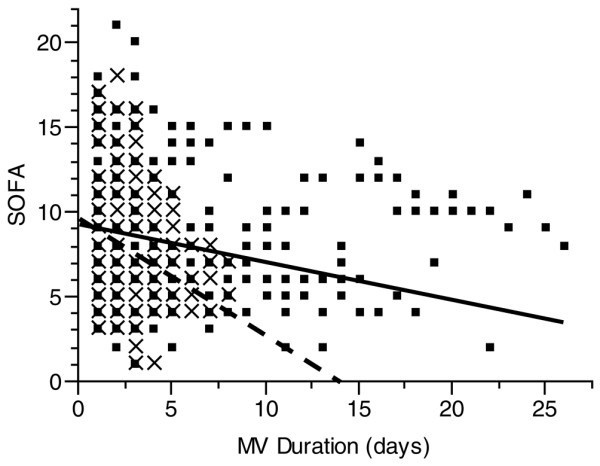
Results: The study was terminated prematurely after 74 patients were enrolled (DIS 36 and SA 38). The two groups had similar age, gender, racial distribution, Acute Physiology and Chronic Health Evaluation II score, and reason for MV. The Data Safety Monitoring Board convened after DIS patients were found to have higher hospital mortality; however, no causal connection between DIS and increased mortality was identified. Interim analysis demonstrated a significant difference in primary endpoint, and study termination was recommended. The DIS group had longer total duration of MV (median 6.7 versus 3.9 days; P = 0.0003), slower improvement of Sequential Organ Failure Assessment over time (0.70 versus 0.23 units per day; P = 0.025), longer ICU length of stay (15 versus 8 days; P < 0.0001), and longer hospital length of stay (23 versus 12 days; P = 0.01).
Conclusion: In our cohort of patients, the use of SA was associated with reduced duration of MV and lengths of stay compared with DIS. Based on these results, DIS may not be appropriate in all mechanically ventilated patients.
Trial registration: ClinicalTrials.gov NCT00205517.
Figures
References
-
- Girard TD, Kress JP, Fuchs BD, Thomason JW, Schweickert WD, Pun BT, Taichman DB, Dunn JG, Pohlman AS, Kinniry PA, Jackson JC, Canonico AE, Light RW, Shintani AK, Thompson JL, Gordon SM, Hall JB, Dittus RS, Bernard GR, Ely EW. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (awakening and breathing controlled trial): a randomised controlled trial. Lancet. 2008;371:126–134. doi: 10.1016/S0140-6736(08)60105-1. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
