

Assessment of surgical skills of trainees in the UK
- PMID: 18492389
- PMCID: PMC2647187
- DOI: 10.1308/003588408X286017
Assessment of surgical skills of trainees in the UK
Abstract
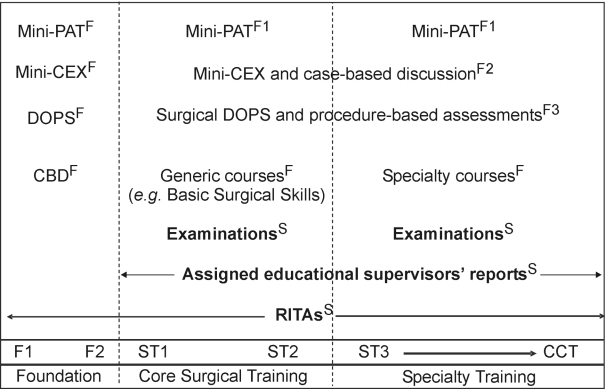
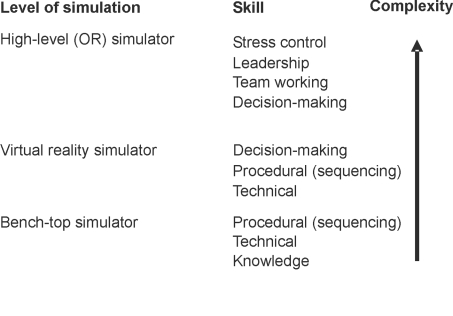
Surgical training and assessment in the UK has been criticised in the past for lacking transparency, reliability and validity. The new Intercollegiate Surgical Curriculum Programme (ISCP) has a well-defined, competence-based syllabus and a system of workplace-based assessments and examinations that map to the syllabus. The main aims of workplace-based assessment are to aid learning through objective feedback and to provide evidence that the competencies required to progress to the next level of training have been achieved. Reduction in surgical experience means that more training will need to be undertaken on simulations, although experience and assessment in the operating room must remains the 'gold-standard'. Simulation training will require the provision of properly resourced surgical skills facilities in every hospital. The key to reliable assessment and constructive feedback is well-trained trainers. Training is a skill that must be learned, and assessment and feedback techniques form part of this. In surgery, it has been assumed that all consultants are trainers but this is clearly not the case. Surgeons will need to follow the example of primary care, where trainers are selected from experienced general practitioners who demonstrate enthusiasm and ability. The reward for the trainer should be protected time for training. The reward for the National Health Service will be better trained surgeons.
Figures
References
-
- Lowry J, Cripps J. Results of the online EWTD trainee survey. Ann R Coll Surg Engl Suppl. 2005;87:86–7.
-
- Rethans J-J, Norcini JJ, Baron-Maldonado M, Blackmore D, Jolly BC, Laduca T, et al. The relationship between competence and performance: implications for assessing practice performance. Med Educ. 2002;36:901–9. - PubMed
-
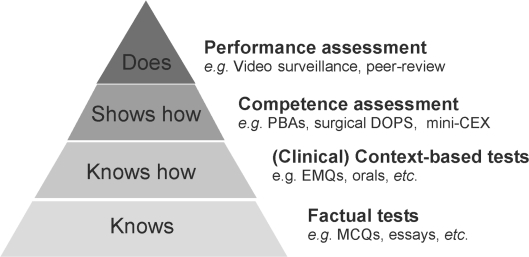
- Miller GE. The assessment of clinical skills, competence and performance. Acad Med Suppl. 1990;65:S63–7. - PubMed
-
- Talbot M. Monkey see, monkey do: a critique of the competency model in graduate medical education. Med Educ. 2004;38:587–92. - PubMed
-
- Schuwirth LWT. Assessing medical competence: finding the right answers. Clin Teacher. 2004;1:14–8.
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous