

Intensity of renal support in critically ill patients with acute kidney injury
- PMID: 18492867
- PMCID: PMC2574780
- DOI: 10.1056/NEJMoa0802639
Intensity of renal support in critically ill patients with acute kidney injury
Erratum in
- N Engl J Med. 2009 Dec 10;361(24):2391
Abstract
Background: The optimal intensity of renal-replacement therapy in critically ill patients with acute kidney injury is controversial.
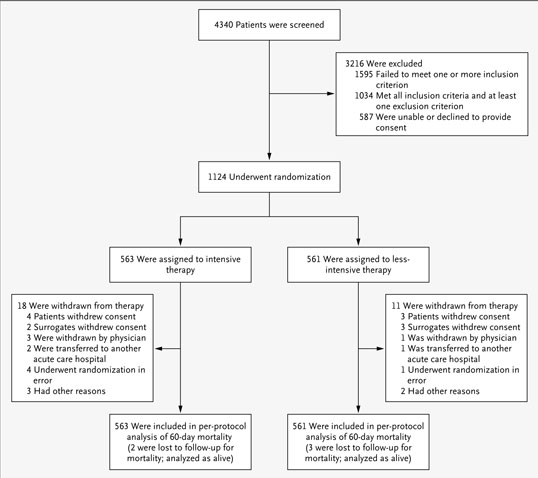
Methods: We randomly assigned critically ill patients with acute kidney injury and failure of at least one nonrenal organ or sepsis to receive intensive or less intensive renal-replacement therapy. The primary end point was death from any cause by day 60. In both study groups, hemodynamically stable patients underwent intermittent hemodialysis, and hemodynamically unstable patients underwent continuous venovenous hemodiafiltration or sustained low-efficiency dialysis. Patients receiving the intensive treatment strategy underwent intermittent hemodialysis and sustained low-efficiency dialysis six times per week and continuous venovenous hemodiafiltration at 35 ml per kilogram of body weight per hour; for patients receiving the less-intensive treatment strategy, the corresponding treatments were provided thrice weekly and at 20 ml per kilogram per hour.
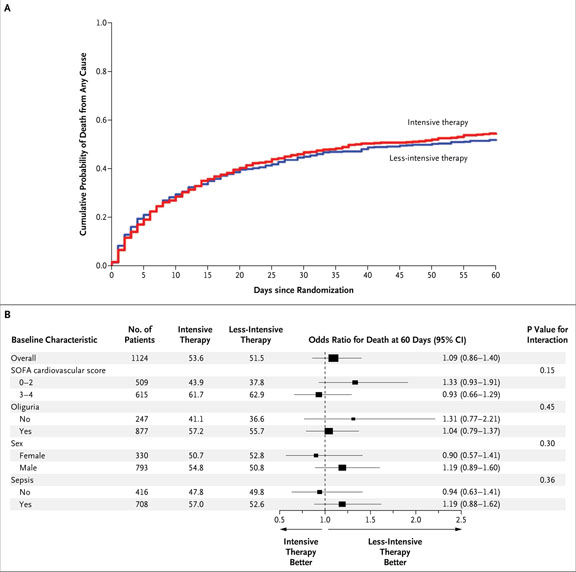
Results: Baseline characteristics of the 1124 patients in the two groups were similar. The rate of death from any cause by day 60 was 53.6% with intensive therapy and 51.5% with less-intensive therapy (odds ratio, 1.09; 95% confidence interval, 0.86 to 1.40; P=0.47). There was no significant difference between the two groups in the duration of renal-replacement therapy or the rate of recovery of kidney function or nonrenal organ failure. Hypotension during intermittent dialysis occurred in more patients randomly assigned to receive intensive therapy, although the frequency of hemodialysis sessions complicated by hypotension was similar in the two groups.
Conclusions: Intensive renal support in critically ill patients with acute kidney injury did not decrease mortality, improve recovery of kidney function, or reduce the rate of nonrenal organ failure as compared with less-intensive therapy involving a defined dose of intermittent hemodialysis three times per week and continuous renal-replacement therapy at 20 ml per kilogram per hour. (ClinicalTrials.gov number, NCT00076219.)
2008 Massachusetts Medical Society
Figures
Comment in
-
Dialysis in acute kidney injury--more is not better.N Engl J Med. 2008 Jul 3;359(1):82-4. doi: 10.1056/NEJMe0803765. Epub 2008 May 20. N Engl J Med. 2008. PMID: 18492868 No abstract available.
-
More-intensive renal replacement therapy has no benefit in critically ill patients with acute kidney injury.Nat Clin Pract Nephrol. 2008 Nov;4(11):596-7. doi: 10.1038/ncpneph0926. Epub 2008 Aug 26. Nat Clin Pract Nephrol. 2008. PMID: 18725914 No abstract available.
-
Dialysis dosing in critically ill patients with acute kidney injury.Am J Kidney Dis. 2008 Oct;52(4):649-52. doi: 10.1053/j.ajkd.2008.07.033. Am J Kidney Dis. 2008. PMID: 18805346 No abstract available.
-
Renal support in critically ill patients with acute kidney injury.N Engl J Med. 2008 Oct 30;359(18):1959; author reply 1961-2. doi: 10.1056/NEJMc081598. N Engl J Med. 2008. PMID: 18971499 No abstract available.
-
Renal support in critically ill patients with acute kidney injury.N Engl J Med. 2008 Oct 30;359(18):1959-60; author reply 1961-2. N Engl J Med. 2008. PMID: 18979569 No abstract available.
-
Renal support in critically ill patients with acute kidney injury.N Engl J Med. 2008 Oct 30;359(18):1960; author reply 1961-2. N Engl J Med. 2008. PMID: 18979570 No abstract available.
-
Renal support in critically ill patients with acute kidney injury.N Engl J Med. 2008 Oct 30;359(18):1960-1. N Engl J Med. 2008. PMID: 18979571 No abstract available.
-
Renal support in critically ill patients with acute kidney injury.N Engl J Med. 2008 Oct 30;359(18):1961; author reply 1961-2. N Engl J Med. 2008. PMID: 18979572 No abstract available.
-
Intensive and less-intensive renal replacement therapy did not differ for death or kidney function in critically ill patients.ACP J Club. 2008 Nov 18;149(5):6. ACP J Club. 2008. PMID: 19014173 No abstract available.
-
Precision Continuous Renal Replacement Therapy and Solute Control.Blood Purif. 2016;42(3):238-47. doi: 10.1159/000448507. Epub 2016 Aug 26. Blood Purif. 2016. PMID: 27562079
References
-
- Nash K, Hafeez A, Hou S. Hospitalacquired renal insufficiency. Am J Kidney Dis. 2002;39:930–6. - PubMed
-
- Liangos O, Wald R, O'Bell JW, Price L, Pereira BJ, Jaber BL. Epidemiology and outcomes of acute renal failure in hospitalized patients: a national survey. Clin J Am Soc Nephrol. 2006;1:43–51. - PubMed
-
- Xue JL, Daniels F, Star RA, et al. Incidence and mortality of acute renal failure in Medicare beneficiaries, 1992 to 2001. J Am Soc Nephrol. 2006;17:1135–42. - PubMed
-
- Waikar SS, Curhan GC, Wald R, Mc-Carthy EP, Chertow GM. Declining mortality in patients with acute renal failure, 1988 to 2002. J Am Soc Nephrol. 2006;17:1143–50. - PubMed
-
- Liaño F, Junco E, Pascual J, Madero R, Verde E. The spectrum of acute renal failure in the intensive care unit compared with that seen in other settings. Kidney Int Suppl. 1998;66:S16–S24. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical