

Successful Multimodality Endoscopic Treatment of Gastric Outlet Obstruction Caused by an Impacted Gallstone (Bouveret's Syndrome)
- PMID: 18493330
- PMCID: PMC2239211
- DOI: 10.1155/2008/471512
Successful Multimodality Endoscopic Treatment of Gastric Outlet Obstruction Caused by an Impacted Gallstone (Bouveret's Syndrome)
Abstract
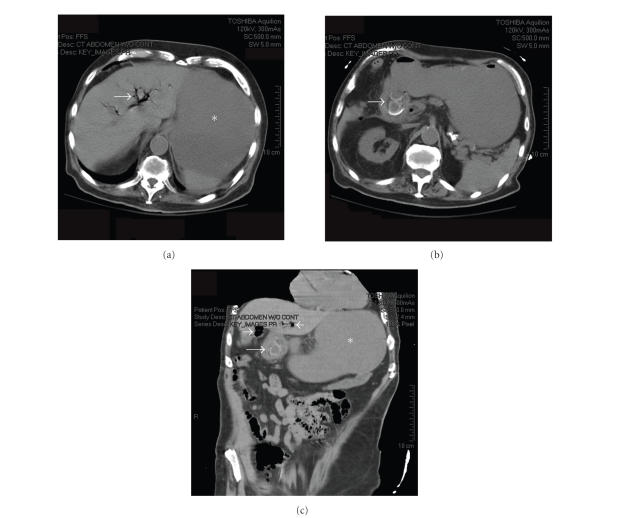
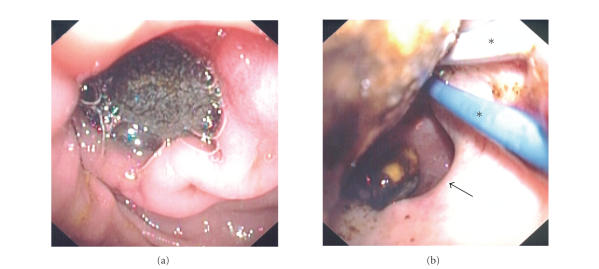
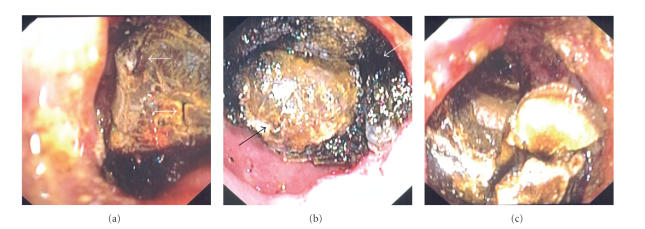
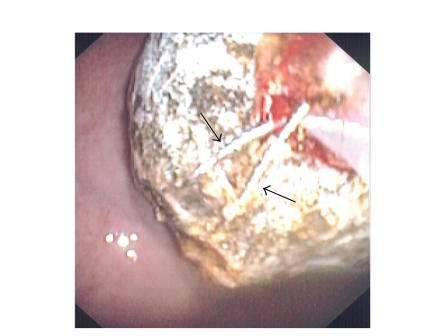
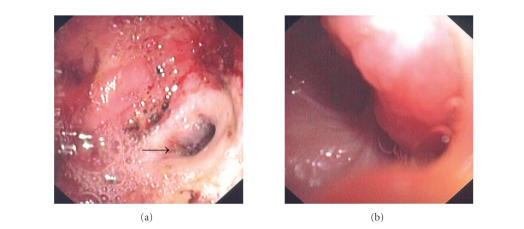
Bouveret's syndrome is a rare condition of gastric outlet obstruction resulting from the migration of a gallstone through a choledochoduodenal fistula. Due to the large size of these stones and the difficult location in which they become impacted, endoscopic treatment is unsuccessful and most patients require surgery. We report the case of an elderly male who presented with nausea and hematemesis, and was found on CT scan and endoscopy to have an obstructing gallstone in his duodenal bulb. After several endoscopic sessions and the use of multiple instruments including a Holmium: YAG laser and electrohydraulic lithotripter, fragmentation and endoscopic removal of the stone were successful. We believe this to be the first case of Bouveret's syndrome successfully treated by endoscopy alone in the United States. We describe the difficulties encountered which necessitated varied and innovative therapeutic techniques.
Figures

References
-
- Lowe AS, Stephenson S, Kay CL, May J. Duodenal obstruction by gallstone (Bouveret's syndrome): a review of the literature. Endoscopy. 2005;37(1):82–87. - PubMed
-
- Bouveret L. Sténose du pylore adhérent à la vésicule. Revue Médicale. 1896;16:1–16.
-
- Bedogni G, Contini S, Meinero M. Pyloroduodenal obstruction due to a biliary stone (Bouveret's syndrome) managed by endoscopic extraction. Gastrointestinal Endoscopy. 1985;31(1):36–38. - PubMed
-
- Moriai T, Hasegawa T, Fuzita M, Kimura A, Tani T, Makino I. Successful removal of massive intragastric gallstones by endoscopic electrohydraulic lithotripsy and mechanical lithotripsy. American Journal of Gastroenterology. 1991;86(5):627–629. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
