

Understanding the impact of male circumcision interventions on the spread of HIV in southern Africa
- PMID: 18493593
- PMCID: PMC2387228
- DOI: 10.1371/journal.pone.0002212
Understanding the impact of male circumcision interventions on the spread of HIV in southern Africa
Abstract
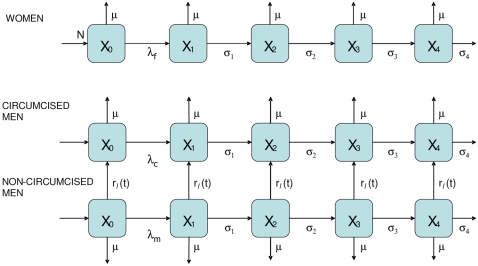
Background: Three randomised controlled trials have clearly shown that circumcision of adult men reduces the chance that they acquire HIV infection. However, the potential impact of circumcision programmes--either alone or in combination with other established approaches--is not known and no further field trials are planned. We have used a mathematical model, parameterised using existing trial findings, to understand and predict the impact of circumcision programmes at the population level.
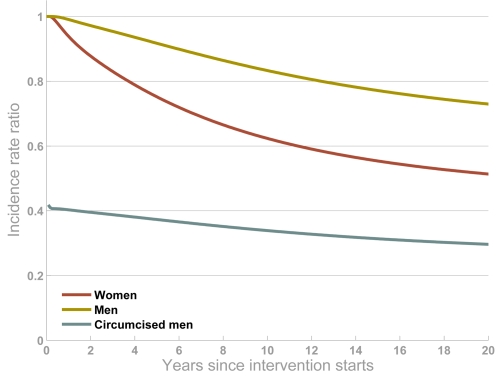
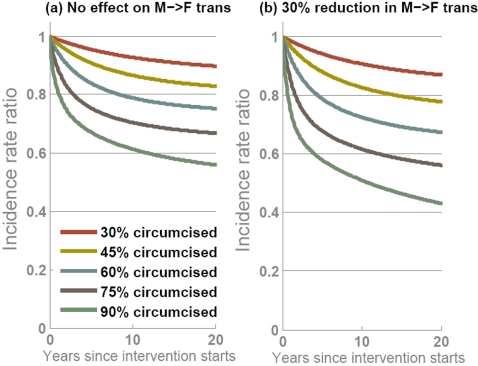
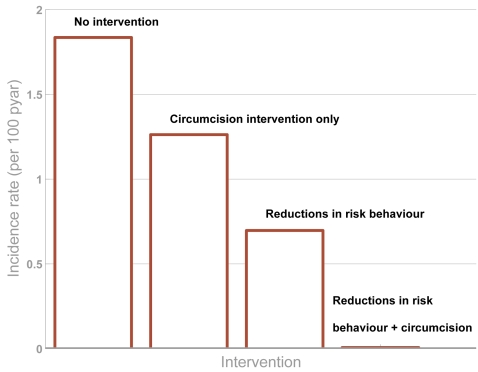
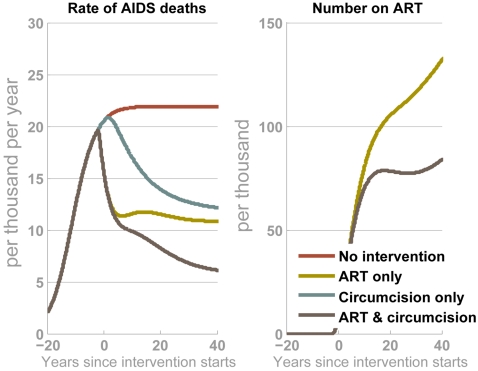
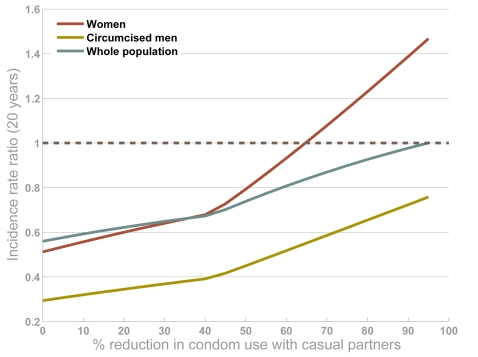
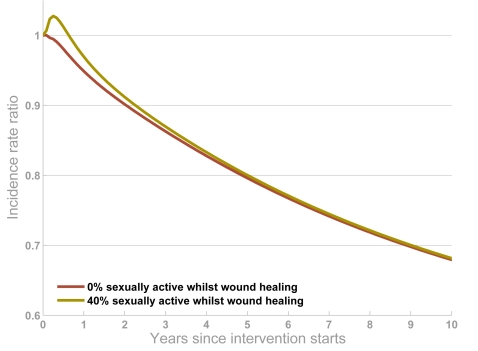
Findings: Our results indicate that circumcision will lead to reductions in incidence for women and uncircumcised men, as well as those circumcised, but that even the most effective intervention is unlikely to completely stem the spread of the virus. Without additional interventions, HIV incidence could eventually be reduced by 25-35%, depending on the level of coverage achieved and whether onward transmission from circumcised men is also reduced. However, circumcision interventions can act synergistically with other types of prevention programmes, and if efforts to change behaviour are increased in parallel with the scale-up of circumcision services, then dramatic reductions in HIV incidence could be achieved. In the long-term, this could lead to reduced AIDS deaths and less need for anti-retroviral therapy. Any increases in risk behaviours following circumcision, i.e. 'risk compensation', could offset some of the potential benefit of the intervention, especially for women, but only very large increases would lead to more infections overall.
Conclusions: Circumcision will not be the silver bullet to prevent HIV transmission, but interventions could help to substantially protect men and women from infection, especially in combination with other approaches.
Conflict of interest statement
Figures
References
-
- UNAIDS, WHO. AIDS Epidemic Update. 2007 (available from http://dataunaidsorg/pub/EPISlides/2007/2007_epiupdate_enpdf).
-
- UNAIDS. Geneva, Switzerland: 1999. Trends in HIV incidence and prevalence: natural course of the epidemic or results of behavioural change?
-
- Kilian AH, Gregson S, Ndyanabangi B, Walusaga K, Kipp W, et al. Reductions in risk behaviour provide the most consistent explanation for declining HIV-1 prevalence in Uganda. Aids. 1999;13:391–398. - PubMed
-
- Stoneburner RL, Low-Beer D. Population-level HIV declines and behavioral risk avoidance in Uganda. Science. 2004;304:714–718. - PubMed
