

Elderly patients with dementia-related symptoms of severe agitation and aggression: consensus statement on treatment options, clinical trials methodology, and policy
- PMID: 18494535
- PMCID: PMC2674239
- DOI: 10.4088/jcp.v69n0602
Elderly patients with dementia-related symptoms of severe agitation and aggression: consensus statement on treatment options, clinical trials methodology, and policy
Abstract
Objective: Atypical antipsychotic drugs have been used off label in clinical practice for treatment of serious dementia-associated agitation and aggression. Following reports of cerebrovascular adverse events associated with the use of atypical antipsychotics in elderly patients with dementia, the U.S. Food and Drug Administration (FDA) issued black box warnings for several atypical antipsychotics titled "Cerebrovascular Adverse Events, Including Stroke, in Elderly Patients With Dementia." Subsequently, the FDA initiated a metaanalysis of safety data from 17 registration trials across 6 antipsychotic drugs (5 atypical antipsychotics and haloperidol). In 2005, the FDA issued a black box warning regarding increased risk of mortality associated with the use of atypical antipsychotic drugs in this patient population.
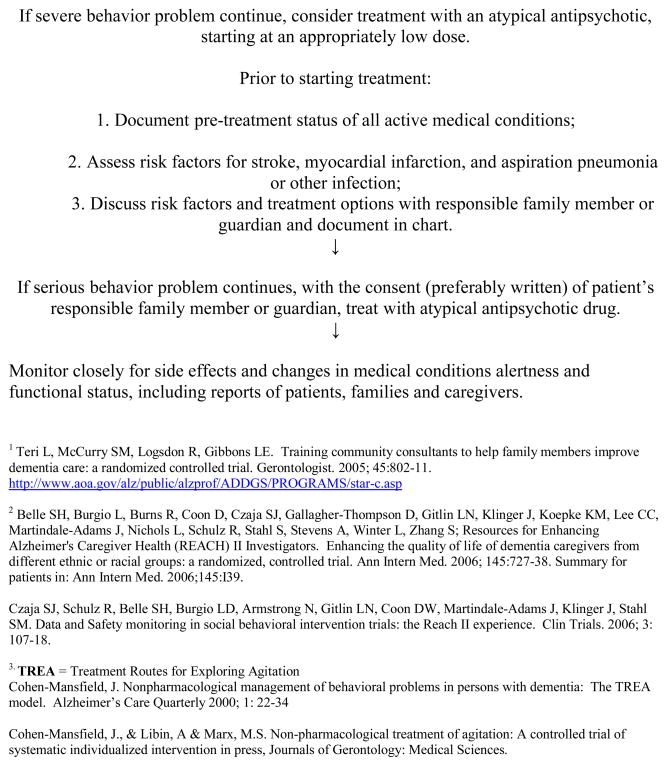
Participants: Geriatric mental health experts participating in a 2006 consensus conference (Bethesda, Md., June 28-29) reviewed evidence on the safety and efficacy of antipsychotics, as well as nonpharmacologic approaches, in treating dementia-related symptoms of agitation and aggression. EVIDENCE/CONSENSUS PROCESS: The participants concluded that, while problems in clinical trial designs may have been one of the contributors to the failure to find a signal of drug efficacy, the findings related to drug safety should be taken seriously by clinicians in assessing the potential risks and benefits of treatment in a frail population, and in advising families about treatment. Information provided to patients and family members should be documented in the patient's chart. Drugs should be used only when nonpharmacologic approaches have failed to adequately control behavioral disruption. Participants also agreed that there is a need for an FDA-approved medication for the treatment of severe, persistent, or recurrent dementia-related symptoms of agitation and aggression (even in the absence of psychosis) that are unresponsive to nonpharmacologic intervention.
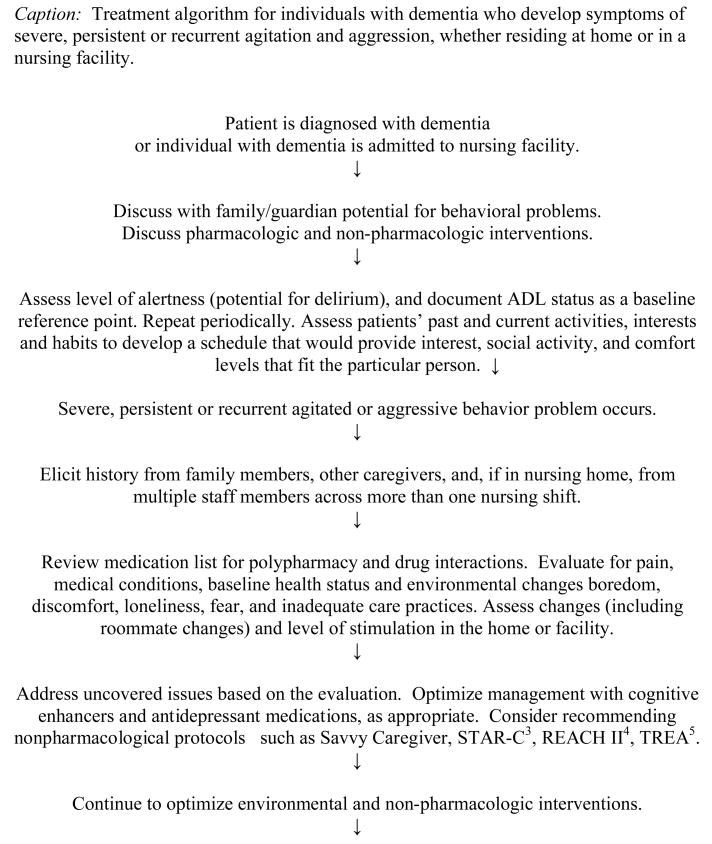
Conclusions: This article outlines methodological enhancements to better evaluate treatment approaches in future registration trials and provides an algorithm for improving the treatment of these patients in nursing home and non-nursing home settings.
Figures
References
-
- Levenson S. Evidence-based practice in LTC: The use of antipsychotics in nursing home residents. Caring for the Ages. 2003. pp. 34–35. Available at: http://www.amda.com/publications/caring/june2003/evidencebased.cfm.
-
- Dolder CR, Jeste DV. Incidence of tardive dyskinesia with typical versus atypical antipsychotics in very high risk patients. Biol Psychiatry. 2003;53:1142–5. - PubMed
-
- Wang PS, Schneeweiss S, Avorn J, et al. Risk of death in elderly users of conventional vs. atypical antipsychotic medications. N Engl J Med. 2005;353:2335–41. - PubMed
-
- Schneider LS, Dagerman KS, Insel P. Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials. JAMA. 2005;294:1934–43. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
