

Evaluation of the nano-oligosaccharide factor lipido-colloid matrix in the local management of venous leg ulcers: results of a randomised, controlled trial
- PMID: 18494623
- PMCID: PMC7951532
- DOI: 10.1111/j.1742-481X.2008.00453.x
Evaluation of the nano-oligosaccharide factor lipido-colloid matrix in the local management of venous leg ulcers: results of a randomised, controlled trial
Abstract
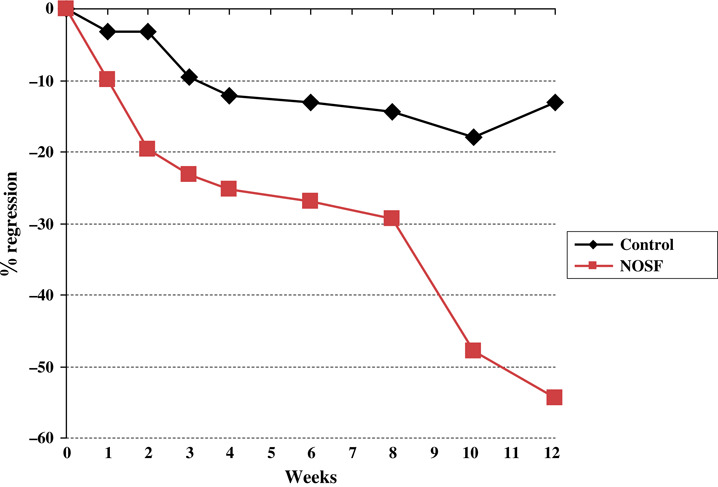
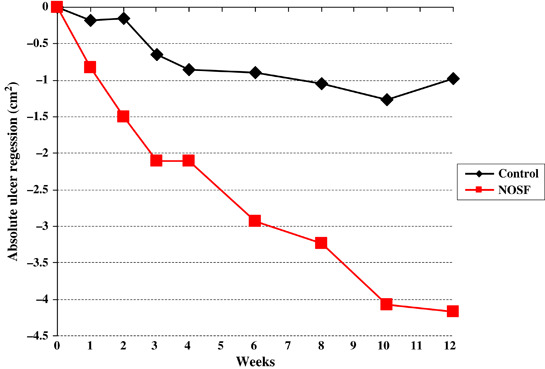
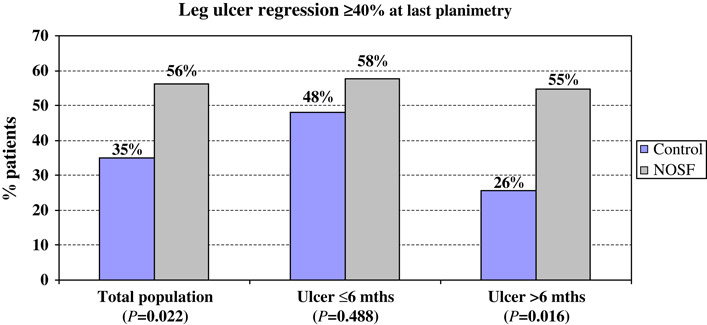
The nano-oligosaccharide factor (NOSF) is a new compound aiming to promote wound closure mainly through inhibition of matrix metalloproteinase (MMP) activity. This factor is incorporated within a lipido-colloid matrix (Techonology Lipido-Colloid-NOSF matrix) and locally released in the wound. The objective of this study was to document the performance (non inferiority or superiority) of the NOSF relative to the Promogran matrix (oxidised regenerated cellulose, ORC) effect in the local management of venous leg ulcers (VLUs). This was a 12-week, open, two-arm, multicentre, randomised study. Patients were selected if the area of their VLU [ankle brachial pressure index >or=0.80] ranged from 5 to 25 cm(2) with a duration >or=3 months. Ulcers had to be free from necrotic tissue. In addition to receiving compression bandage therapy, patients were randomly allocated to either NOSF matrix or ORC treatment for 12 weeks. The VLUs were assessed on a weekly basis and wound tracings were recorded. Percentage wound relative reduction (%RR) was the primary efficacy criterion. Secondary objectives were wound absolute reduction (AR), healing rate (HR) and % of wounds with >or=40% reduction compared with baseline. A total of 117 patients were included (57 NOSF matrix and 60 ORC). Mean population age was 71.3 +/- 13.5 years, body mass index was >or=30 kg/m(2) in 39.3% and 15.4% were diabetics. Fifty-six per cent of the VLUs were present for >6 months, 61% were recurrent and 68% were stagnating despite appropriate care. Mean wound area at baseline was 11.2 +/- 7.4 cm(2). At the last evaluation, mean difference between the groups for %RR was 33.6 +/- 15.0% in favour of NOSF matrix with a unilateral 95% confidence interval (CI) lower limit of 8.6% not including the null value. Therefore, a superiority of NOSF matrix effect compared with ORC was concluded (P = 0.0059 for superiority test). The median of the wound area reduction was 61.1% and 7.7% in the NOSF matrix and control groups, respectively (per-protocol analysis), or 54.4% versus 12.9% in intent-to-treat analysis (p = 0.0286). Median AR was 4.2 cm(2) in the NOSF group and 1.0 cm(2) with ORC (P = 0.01). Median HR was -0.056 and -0.015 cm(2)/day in NOSF and ORC groups, respectively (P = 0.029). By logistic regression, the NOSF versus control odds ratio to reach 40% area reduction was 2.4 (95% CI: 1.1-5.3; P = 0.026). In the oldest and largest VLUs, a strong promotion of healing effect was particularly observed in the NOSF matrix group compared with the control group. NOSF matrix is a very promising option for the local management of chronic wounds, especially for VLUs with poor healing prognosis.
Figures
References
-
- Nelzen O, Bergqvist D, Lindhagen A. Venous and non‐venous leg ulcers: clinical history and appearance in a population study. Br J Surg 1994;81:182–7. - PubMed
-
- Graham ID, Harrison MB, Nelson EA, Lorimer K, Fisher A. Prevalence of lower‐limb ulceration: a systematic review of prevalence studies. Adv Skin Wound Care 2003;16:305–16. - PubMed
-
- Walker NK, Vandal AC, Holden JK, Rodgers A, Birchall N, Norton R, Triggs CM, MacMahon S. Does capture‐recapture analysis provide more reliable estimates of the incidence and prevalence of leg ulcers in the community? Aust N Z J Public Health 2002;26:451–5. - PubMed
-
- Marklund B, Sulau T, Lindholm C. Prevalence of non‐healed and healed chronic leg ulcers in an elderly rural population. Scand J Prim Health Care 2000;18:58–60. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
