

Delirium in the intensive care unit
- PMID: 18495054
- PMCID: PMC2391269
- DOI: 10.1186/cc6149
Delirium in the intensive care unit
Abstract
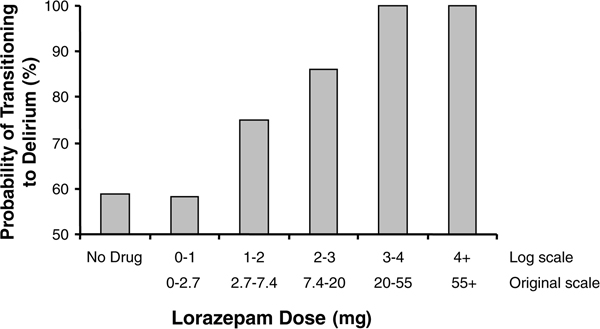
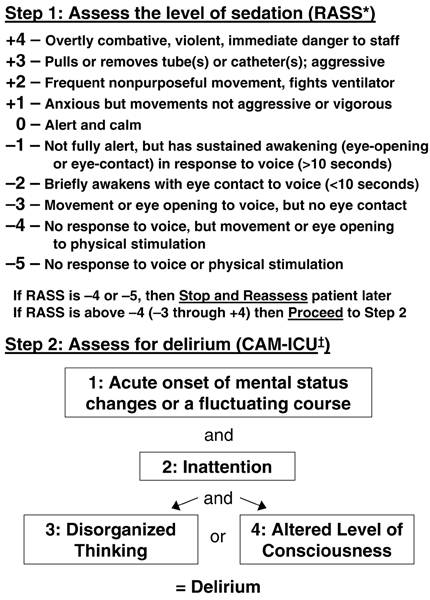
Delirium, an acute and fluctuating disturbance of consciousness and cognition, is a common manifestation of acute brain dysfunction in critically ill patients, occurring in up to 80% of the sickest intensive care unit (ICU) populations. Critically ill patients are subject to numerous risk factors for delirium. Some of these, such as exposure to sedative and analgesic medications, may be modified to reduce risk. Although dysfunction of other organ systems continues to receive more clinical attention, delirium is now recognized to be a significant contributor to morbidity and mortality in the ICU, and it is recommended that all ICU patients be monitored using a validated delirium assessment instrument. Patients with delirium have longer hospital stays and lower 6-month survival than do patients without delirium, and preliminary research suggests that delirium may be associated with cognitive impairment that persists months to years after discharge. Little evidence exists regarding the prevention and treatment of delirium in the ICU, but multicomponent interventions reduce the incidence of delirium in non-ICU studies. Strategies for the prevention and treatment of ICU delirium are the subjects of multiple ongoing investigations.
Figures
References
-
- The Nature and Extent of Medical Injury in Older Patients http://assets.aarp.org/rgcenter/health/2000_17_injury.pdf
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
