

Accurate characterization of extravascular lung water in acute respiratory distress syndrome
- PMID: 18496374
- PMCID: PMC2713576
- DOI: 10.1097/CCM.0b013e3181743eeb
Accurate characterization of extravascular lung water in acute respiratory distress syndrome
Abstract
Objectives: Measurements of extravascular lung water (EVLW) correlate to the degree of pulmonary edema and have substantial prognostic information in critically ill patients. Prior studies using single indicator thermodilution have reported that 21% to 35% of patients with clinical acute respiratory distress syndrome (ARDS) have normal EVLW (<10 mL/kg). Given that lung size is independent of actual body weight, we sought to determine whether indexing EVLW to predicted or adjusted body weight affects the frequency of increased EVLW in patients with ARDS.
Design: Prospective, observational cohort study.
Setting: Medical and surgical intensive care units at two academic hospitals.
Patients: Thirty patients within 72 hrs of meeting American-European Consensus Conference definition of ARDS and 14 severe sepsis patients without ARDS.
Interventions: None.
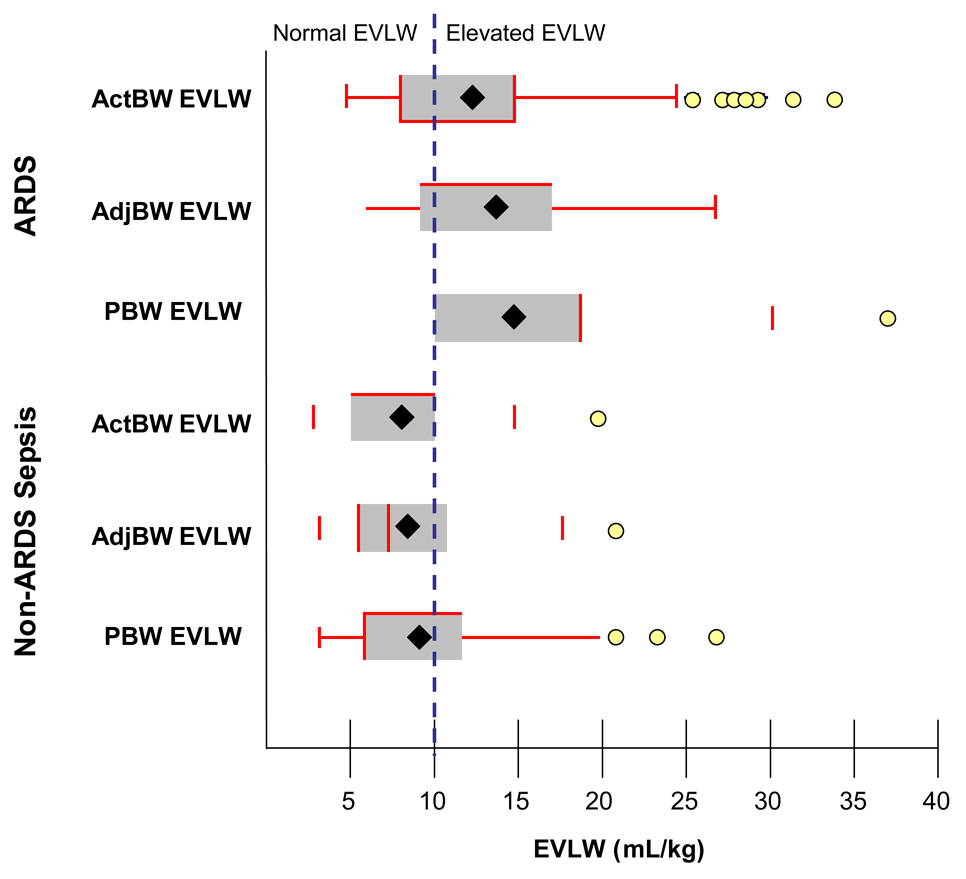
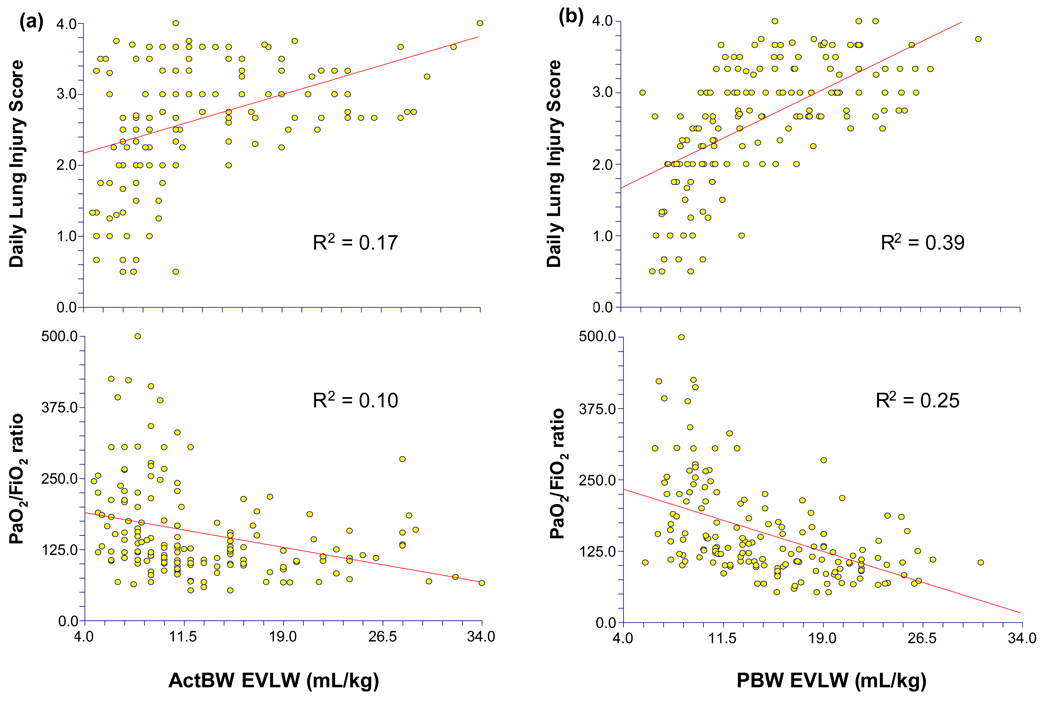
Measurement and main results: EVLW was measured for 7 days by PiCCO transpulmonary thermodilution; 225 measurements of EVLW indexed to actual body weight (ActBW) were compared with EVLW indexed to predicted body weight (PBW) and adjusted body weight (AdjBW). Mean EVLW indexed to ActBW was 12.7 mg/kg for ARDS patients and 7.8 mg/kg for non-ARDS sepsis patients (p < .0001). In all patients, EVLW increased an average of 1.1 +/- 2.1 mL/kg when indexed to AdjBW and 2.0 +/- 4.1 mL/kg when indexed to PBW. Indexing EVLW to PBW or AdjBW increased the proportion of ARDS patients with elevated EVLW (each p < .05) without increasing the frequency of elevated EVLW in non-ARDS patients. EVLW indexed to PBW had a stronger correlation to Lung Injury Score (r2 = .39 vs. r2 = .17) and PaO2/FiO2 ratio (r2 = .25 vs. r2 = .10) than did EVLW indexed to ActBW.
Conclusions: Indexing EVLW to PBW or AdjBW reduces the number of ARDS patients with normal EVLW and correlates better to Lung Injury Score and oxygenation than using ActBW. Studies are needed to confirm the presumed superiority of this method for diagnosing ARDS and to determine the clinical treatment implications.
Figures
Comment in
-
Is extravascular lung water measurement in acute respiratory distress syndrome worth the effort?Crit Care Med. 2008 Jun;36(6):1970. doi: 10.1097/CCM.0b013e318176a92c. Crit Care Med. 2008. PMID: 18520658 No abstract available.
References
-
- Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353:1685–1693. - PubMed
-
- Doyle RL, Szaflarski N, Modin GW, Wiener-Kronish JP, Matthay MA. Identification of patients with acute lung injury. Predictors of mortality. Am J Respir Crit Care Med. 1995;152:1818–1824. - PubMed
-
- Zilberberg M, Epstein S. Acute Lung Injury in the Medical ICU . Comorbid Conditions, Age, Etiology, and Hospital Outcome. American Journal of Respiratory and Critical Care Medicine. 1998;157:1159–1164. - PubMed
-
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994;149:818–824. - PubMed
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342:1334–1349. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
