

Postconditioning with isoflurane reduced ischemia-induced brain injury in rats
- PMID: 18497606
- PMCID: PMC2666347
- DOI: 10.1097/ALN.0b013e3181730257
Postconditioning with isoflurane reduced ischemia-induced brain injury in rats
Abstract
Background: Preexposure of brain to isoflurane, a commonly used anesthetic, induces ischemic tolerance. This phenomenon is called isoflurane preconditioning. However, it is not known whether isoflurane application after ischemia provides neuroprotection.
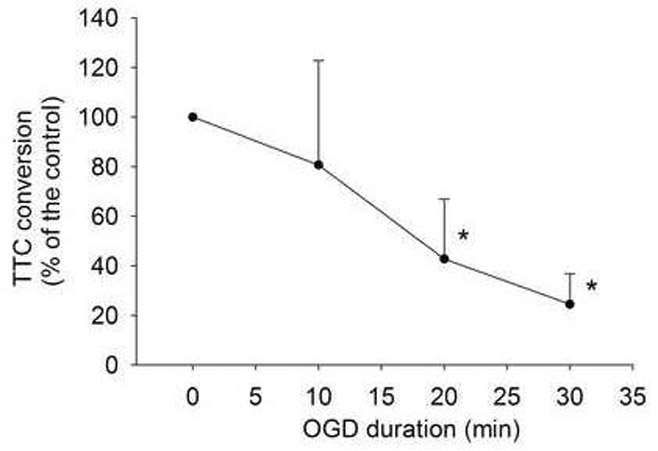
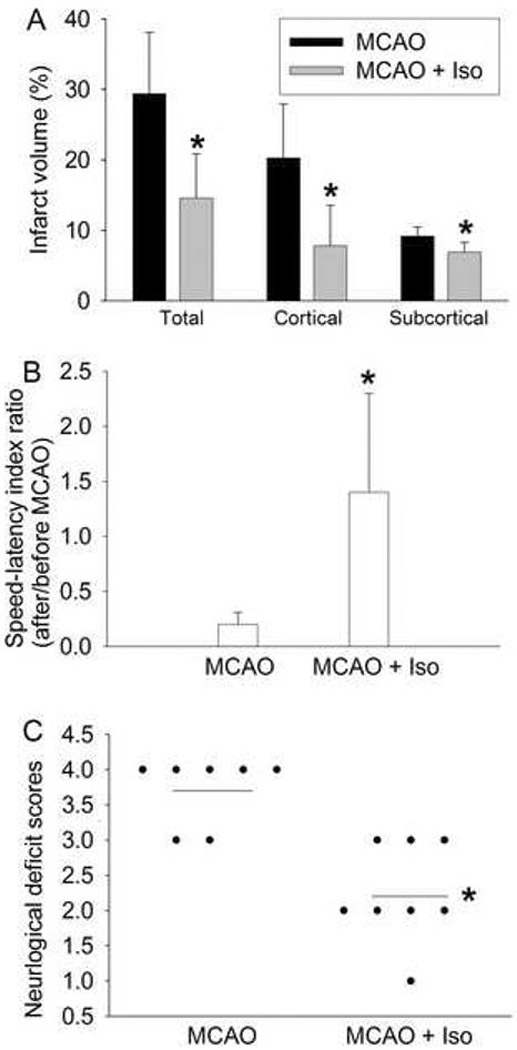
Methods: Corticostriatal slices (400 microm) freshly prepared from adult male Sprague-Dawley rats were subjected to a 15-min oxygen-glucose deprivation (OGD; to simulate ischemia in vitro). Isoflurane was applied after OGD. Brain slices were harvested 2 h after OGD for measuring 2,3,5-triphenyltetrazolium chloride (TTC) conversion to quantify cell injury. Adult male Sprague-Dawley rats were also subjected to middle cerebral arterial occlusion for 90 min and then treated with or without 2% isoflurane for 60 min started at the onset of reperfusion. The infarct volumes, neurologic deficit scores, and performance on rotarod were evaluated at 24 h after the onset of reperfusion.
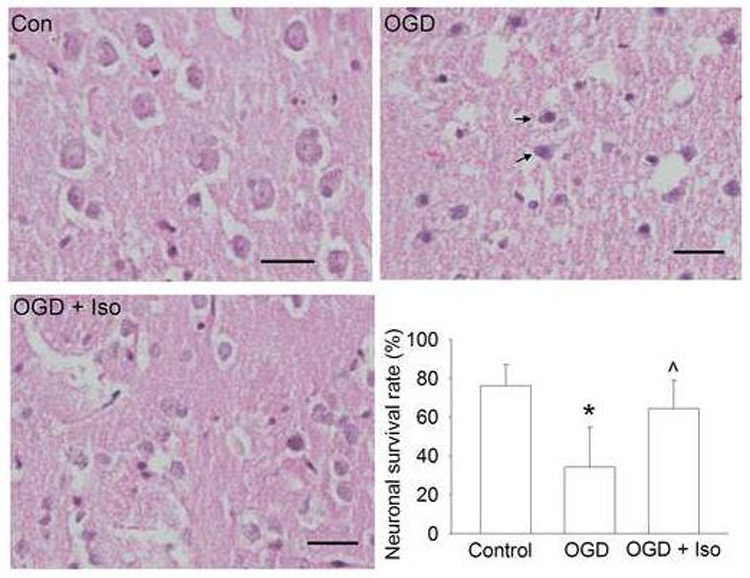
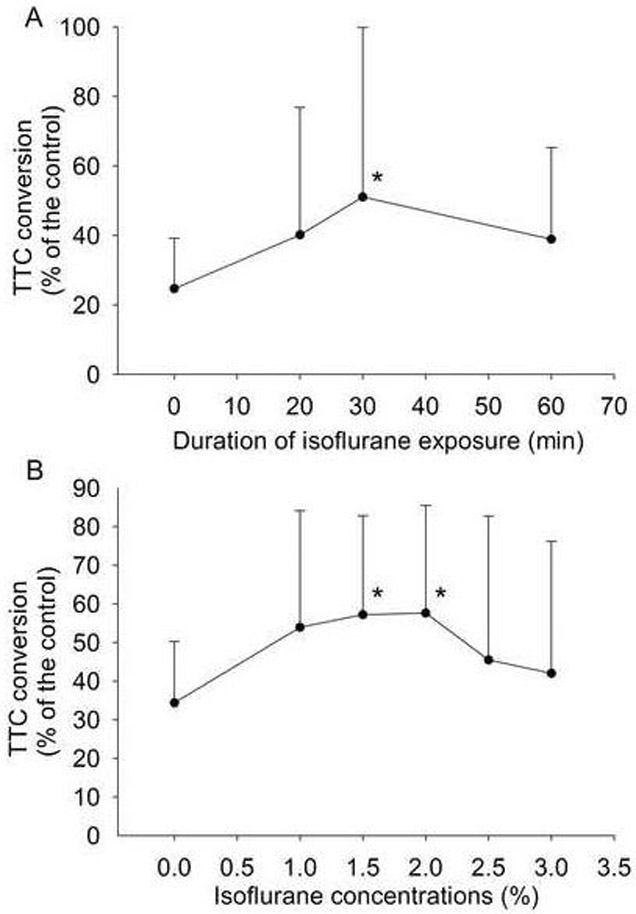
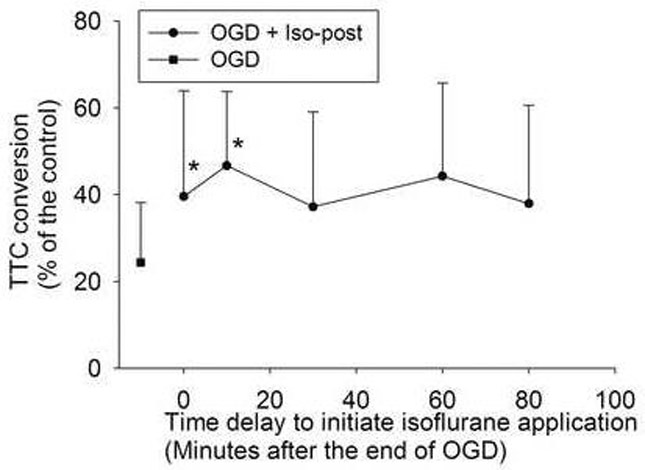
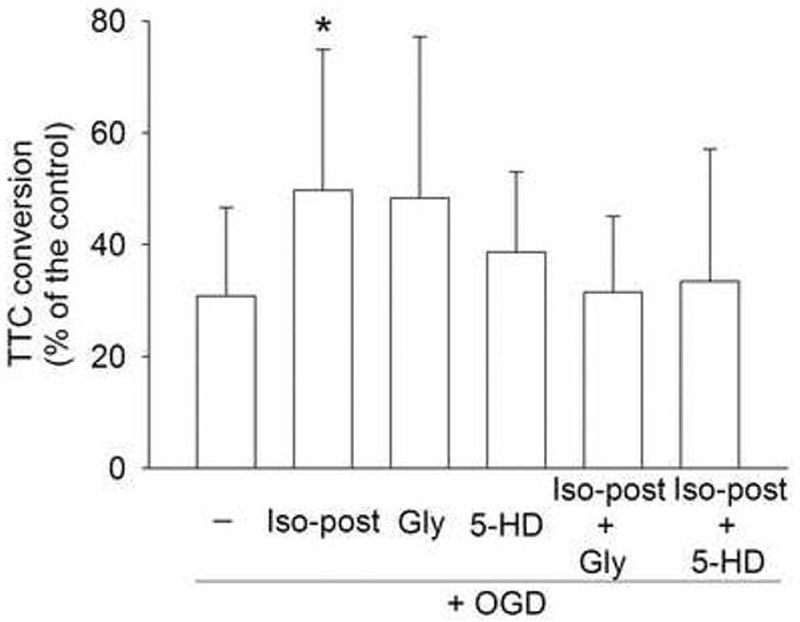
Results: Isoflurane applied immediately after the 15-min OGD for 30 min dose-dependently reversed the OGD-induced decrease of TTC conversion. The TTC conversion was 34 +/- 16% and 58 +/- 28% of the control, respectively, for OGD alone and OGD plus 2% isoflurane (P < 0.05, n = 12). Application of 2% isoflurane for 30 min started at 10 min after the OGD also reduced the OGD-decreased TTC conversion. The presence of 0.3 microm glibenclamide, a general adenosine 5'-triphosphate-sensitive potassium channel blocker, or 500 microm 5-hydroxydecanoic acid, a mitochondrial adenosine 5'-triphosphate-sensitive potassium channel blocker, during the application of 2% isoflurane abolished the isoflurane preservation of TTC conversion. Application of isoflurane during reperfusion also improved neurologic outcome after brain ischemia.
Conclusions: The results suggest that isoflurane administrated after OGD or brain ischemia provides neuroprotection. Mitochondrial adenosine 5'-triphosphate-sensitive potassium channels may be involved in this protection.
Figures
References
-
- Martin JA, Smith BL, Matthews TJ, Ventura SJ. Births and Deaths: Preliminary Data for 1998. National Vital Statistics Reports. 1999;47:1–45. - PubMed
-
- Ferrari R, Ceconi C, Curello S, Percoco G, Toselli T, Antonioli G. Ischemic preconditioning, myocardial stunning, and hibernation: basic aspects. American Heart Journal. 1999;138:S61–8. - PubMed
-
- Tomai F, Crea F, Chiariello L, Gioffre PA. Ischemic preconditioning in humans: models, mediators, and clinical relevance. Circulation. 1999;100:559–63. - PubMed
-
- Zheng S, Zuo Z. Isoflurane preconditioning induces neuroprotection against ischemia via activation of p38 mitogen-activated protein kinase. Molecular Pharmacology. 2004;65:1172–80. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
