

Challenges in using opioids to treat pain in persons with substance use disorders
- PMID: 18497713
- PMCID: PMC2797112
- DOI: 10.1151/ascp08424
Challenges in using opioids to treat pain in persons with substance use disorders
Abstract
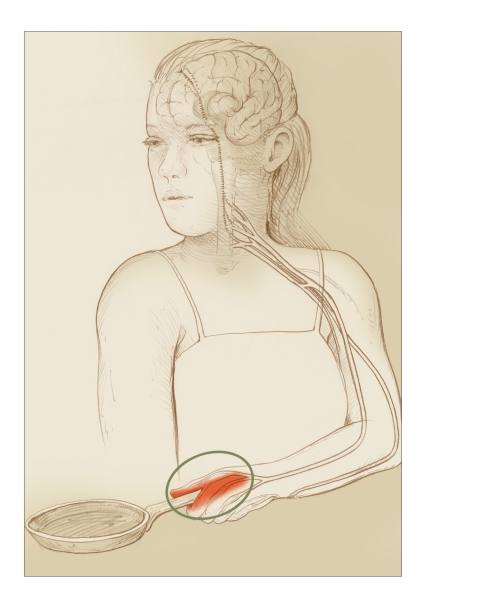
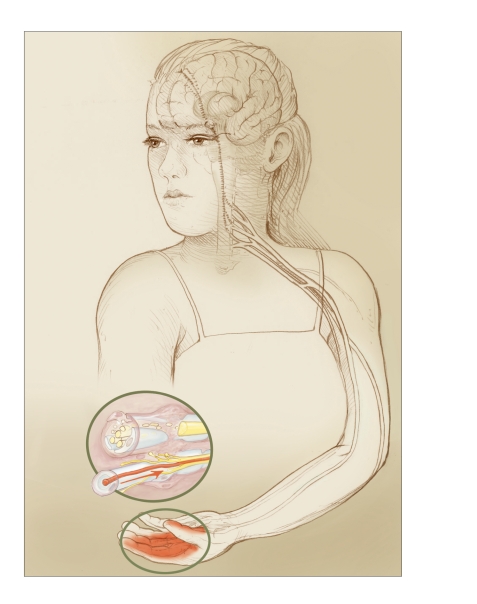
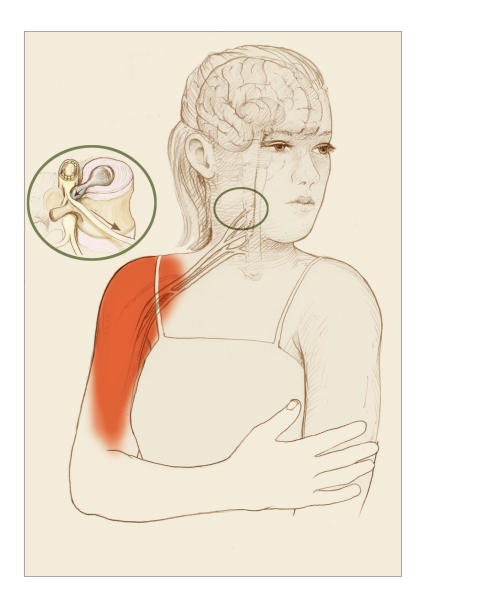
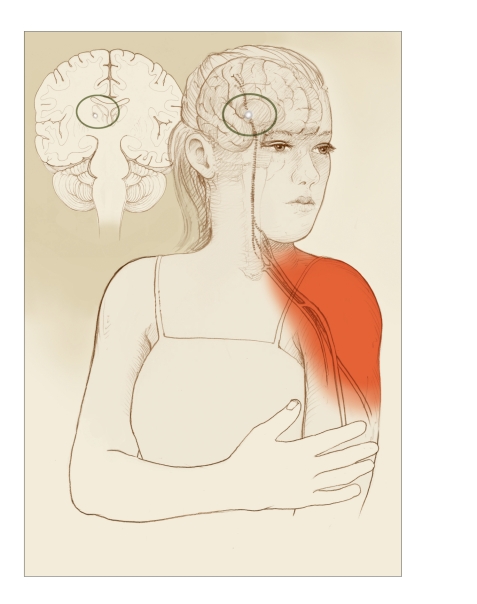
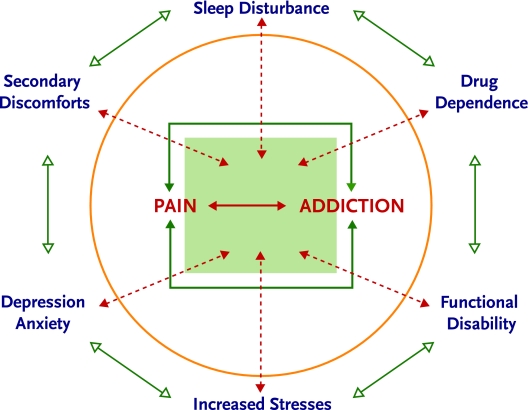
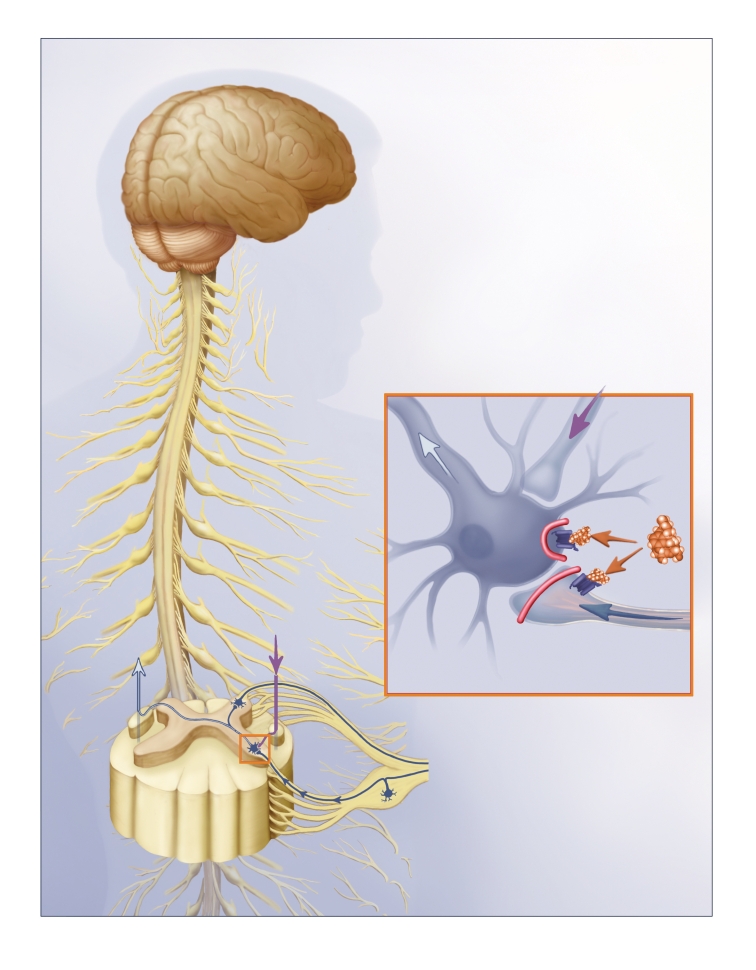
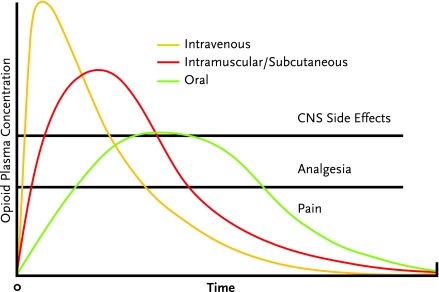
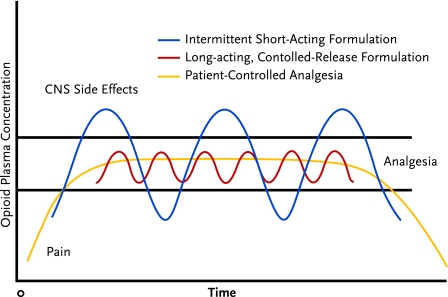
Pain and substance abuse co-occur frequently, and each can make the other more difficult to treat. A knowledge of pain and its interrelationships with addiction enhances the addiction specialist's efficacy with many patients, both in the substance abuse setting and in collaboration with pain specialists. This article discusses the neurobiology and clinical presentation of pain and its synergies with substance use disorders, presents methodical approaches to the evaluation and treatment of pain that co-occurs with substance use disorders, and provides practical guidelines for the use of opioids to treat pain in individuals with histories of addiction. The authors consider that every pain complaint deserves careful investigation and every patient in pain has a right to effective treatment.
Figures
Comment in
-
Response: providing relief, avoiding euphoria.Addict Sci Clin Pract. 2008 Jun;4(2):26-7. doi: 10.1151/ascp084226. Addict Sci Clin Pract. 2008. PMID: 18497714 Free PMC article. No abstract available.
References
-
- Acosta M, Haller DL. Psychiatric and substance abuse comorbidity influences treatment outcomes in opioid-abusing patients. Paper presented at the College on Problems of Drug Dependency annual meeting; Scottsdale, AZ. 2006.
-
- Adams NJ, et al. Opioids and the treatment of chronic pain in a primary care sample. Journal of Pain and Symptom Management. 2001;22(3):791–796. - PubMed
-
- Akbik H, et al. Validation and clinical application of the Screener and Opioid Assessment for Patients with Pain (SOAPP) Journal of Pain and Symptom Management. 2006;32(3):287–293. - PubMed
-
- Amabile CM, Bowman BJ. Overview of oral modified-release opioid products for the management of chronic pain. The Annals of Pharmacotherapy. 2006;40(7–8):1327–1335. - PubMed
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed., Text Revision. Washington, DC: American Psychiatric Association; 2000. DSM-IV-TR.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical