

Surgeons' beliefs and perceptions about removal of orthopaedic implants
- PMID: 18501014
- PMCID: PMC2430567
- DOI: 10.1186/1471-2474-9-73
Surgeons' beliefs and perceptions about removal of orthopaedic implants
Abstract
Background: The routine removal of orthopaedic fixation devices after fracture healing remains an issue of debate. There are no evidence-based guidelines on this matter, and little is known on surgeons' practice and perceived effectiveness of implant removal in different clinical settings.
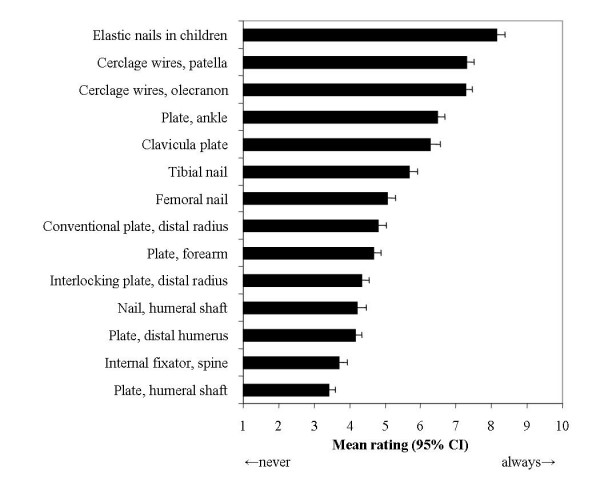
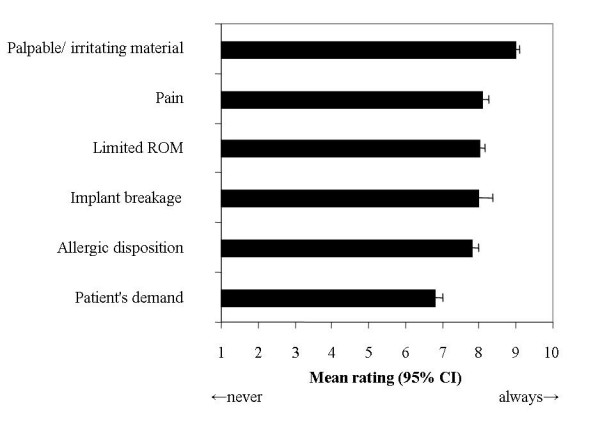
Methods: A 41-item questionnaire was distributed to 730 attendees of the AO Principles and Masters Courses of Operative Fracture Treatment in Davos, Switzerland, to assess their attitudes towards removal of different types of implants, and perceived benefits and risks with this common procedure.
Results: The response rate was 655/730 (89.7%), representing 54.6% of all 1199 course attendees. Surgeons from 65 countries (571 males and 84 females, mean age 39 +/- SD 9 years) took part in the survey. Fifty-eight percent of the participants did not agree that routine implant removal is necessary, and 49% and 58% did not agree that indwelling implants pose an excess risk for fractures or general adverse effects. Forty-eight percent felt that removal is riskier than leaving the implant in situ. Implant removal in symptomatic patients was rated to be moderately effective (mean rating on a 10-point-scale, 5.8, 95% confidence interval 5.7-6.0). Eighty-five percent of all participants agreed that implant removal poses a burden to hospital resources. Surgeons were undetermined whether implant removal is adequately reimbursed by payers of health care services (44% "I-don't-know"-answers).
Conclusion: Many surgeons refuse a routine implant removal policy, and do not believe in clinically significant adverse effects of retained metal implants. Given the frequency of the procedure in orthopaedic departments worldwide, there is an urgent need for a large randomized trial to determine the efficacy and effectiveness of implant removal with regard to patient-centred outcomes.
Figures
References
-
- Bostman O, Pihlajamaki H. Routine implant removal after fracture surgery: a potentially reducible consumer of hospital resources in trauma units. J Trauma. 1996;41:846–849. - PubMed
-
- Davison BL. Refracture following plate removal in supracondylar-intercondylar femur fractures. Orthopedics. 2003;26:157–159. - PubMed
-
- Langkamer VG, Ackroyd CE. Removal of forearm plates. A review of the complications. J Bone Joint Surg Br. 1990;72:601–604. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
