

Review
doi: 10.1016/j.pcl.2008.02.016.
Surfactant for pediatric acute lung injury
Affiliations
- PMID: 18501754
- PMCID: PMC4275446
- DOI: 10.1016/j.pcl.2008.02.016
Item in Clipboard
Review
Surfactant for pediatric acute lung injury
Pediatr Clin North Am.
2008 Jun.
Abstract
This article reviews exogenous surfactant therapy and its use in mitigating acute lung injury (ALI) and the acute respiratory distress syndrome (ARDS) in infants, children, and adults. Biophysical and animal research documenting surfactant dysfunction in ALI/ARDS is described, and the scientific rationale for treatment with exogenous surfactant is discussed. Major emphasis is placed on reviewing clinical studies of surfactant therapy in pediatric and adult patients who have ALI/ARDS. Particular advantages from surfactant therapy in direct pulmonary forms of these syndromes are described. Also discussed are additional factors affecting the efficacy of exogenous surfactants in ALI/ARDS.
Figures
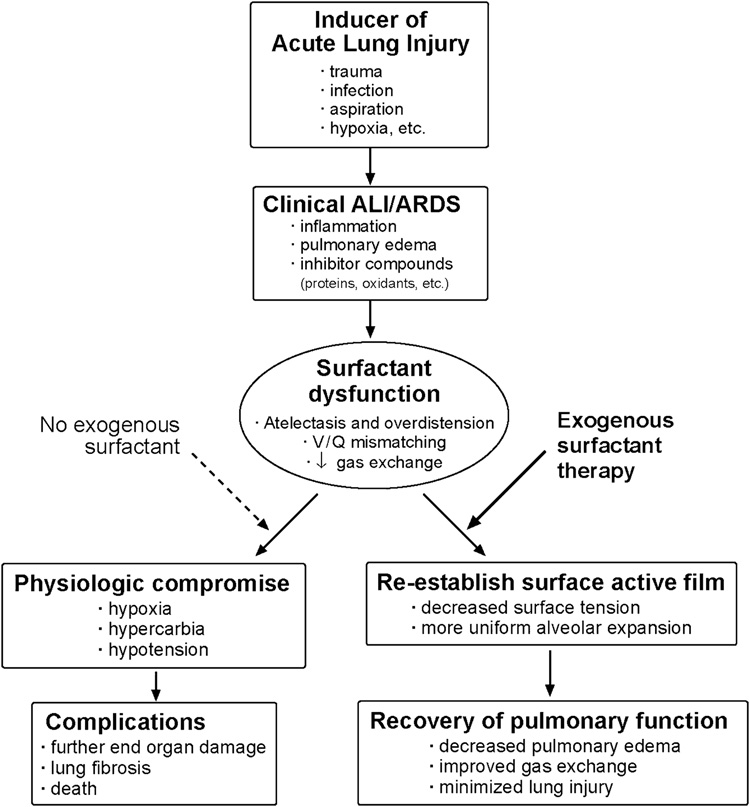
The pathophysiology of acute inflammatory lung injury includes surfactant dysfunction, which contributes to respiratory failure in term infants, children, and adults with clinical acute lung injury (ALI) and the acute respiratory distress syndrome (ARDS). Surfactant dysfunction reduces lung volumes and compliance, causes atelectasis and overdistension, increases ventilation/perfusion (V/Q) mismatching, and reduces gas exchange. In addition, surfactant dysfunction and lung injury can also be present in the clinical course of premature infants being treated with mechanical ventilation and supplemental oxygen for surfactant deficient lung disease in association with the neonatal respiratory distress syndrome (RDS). Scientific understanding indicates that surfactant dysfunction in lung injury can, at least in principle, be ameliorated by exogenous surfactant therapy as discussed in this article.
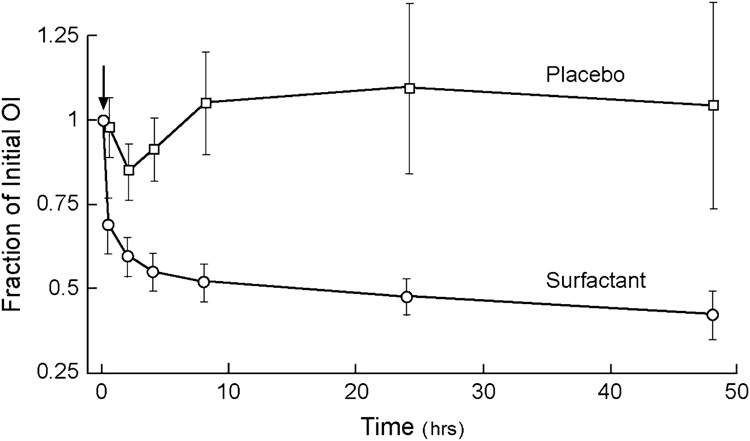
Patients ranging in age from 1 day through 18 years in eight pediatric intensive care units were randomized to surfactant or control groups. Surfactant-treated patients received a dose of Infasurf® of 80 mL/m2 body surface (70 mg/kg body weight) by tracheal instillation during hand-ventilation with 100% oxygen (arrow). Control patients received hand-ventilation and 100% oxygen alone. Ten of 21 surfactant-treated patients received a second dose 12 or more hours after the first. Significant improvements were found in lung function in patients receiving exogenous surfactant therapy. OI is defined as: 100 × MAP × FiO2/PaO2, where MAP = mean airway pressure; FiO2 = fraction of inspired oxygen; PaO2 = arterial partial pressure of oxygen. Data from Willson et al [125].
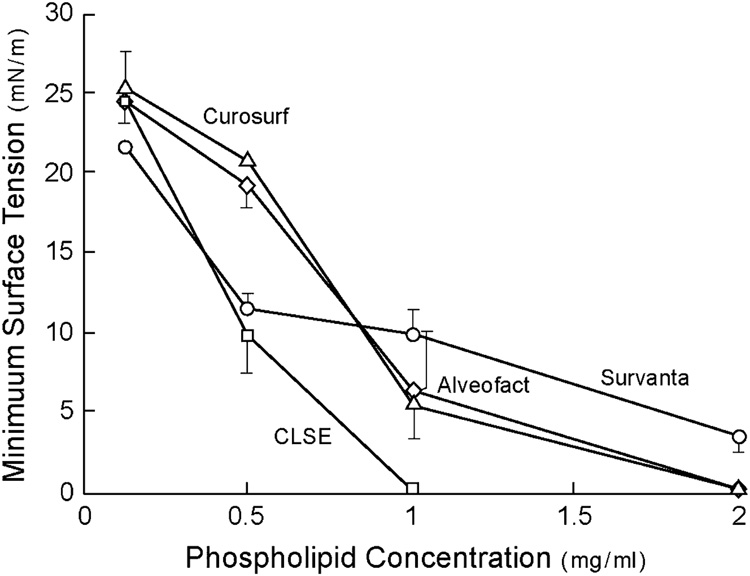
Minimum surface tension after 5 minutes of pulsation in a bubble surfactometer (37°C, 20 cycles/min, 50% area compression) is plotted as a function of surfactant phospholipid concentration for several clinical surfactants. The surfactants shown vary widely in overall surface tension lowering ability, with the most active being Category I surfactants from Table 3 (e.g., Infasurf® and Alveofact®). Data redrawn from Seeger et al [51].
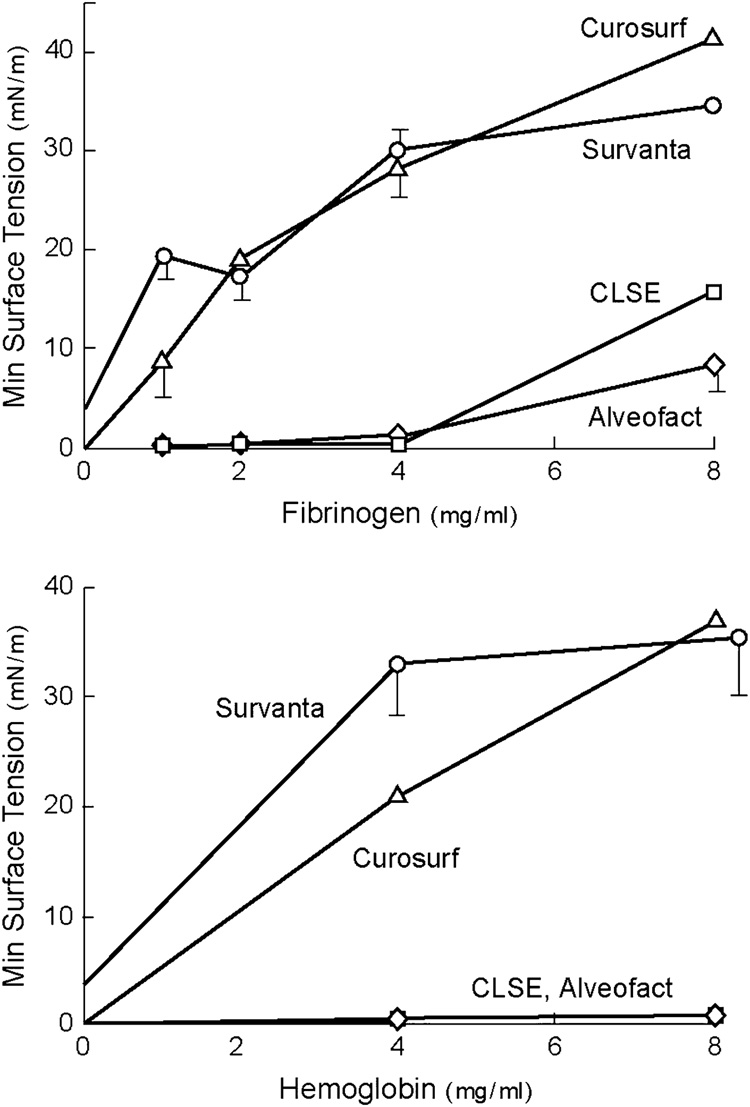
Minimum surface tension after 5 minutes of pulsation in a bubble surfactometer (37°C, 20 cycles/min, and 50% area compression) is plotted against the concentration of inhibitory blood proteins (fibrinogen and hemoglobin). The results indicate that animal-derived exogenous surfactants that closely mimic natural surfactant by being extracted from lung lavage (Category I surfactants from Table 3) have an improved ability to resist inhibition by plasma proteins compared to the other preparations shown. Surfactant phospholipid concentration was 2 mg/ml. Redrawn from [51].
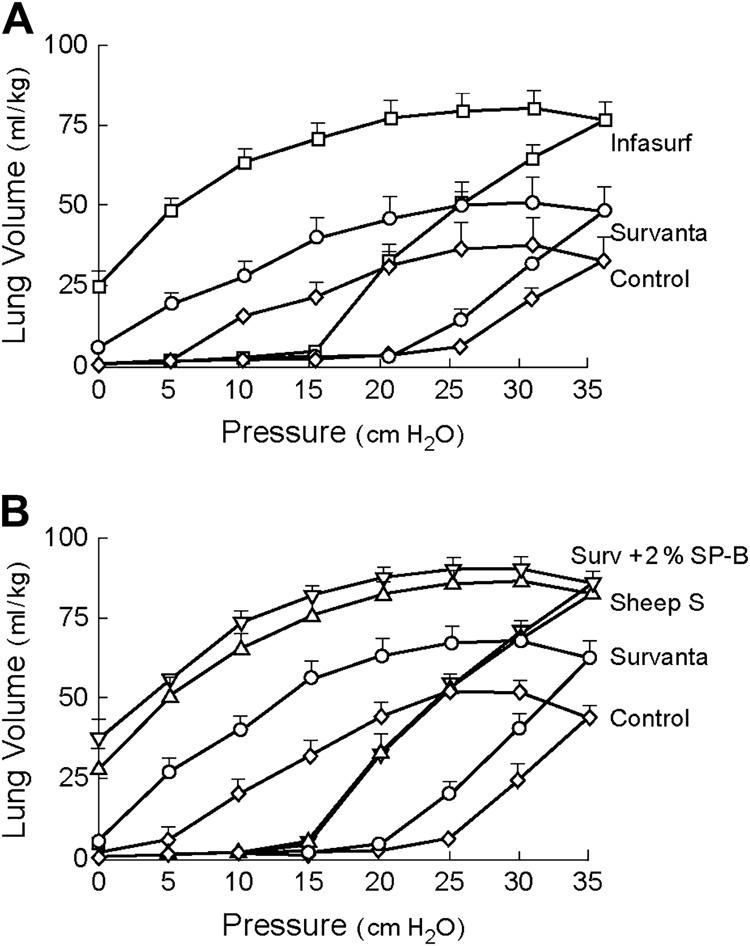
(Top ): Premature rabbit fetuses (27 days gestation) treated with Survanta® or Infasurf®, and untreated controls; (Bottom ): Premature rabbit fetuses treated with Survanta®, Survanta® + SP-B (2% by wt by ELISA), natural surfactant from adult sheep (Sheep S), or untreated controls. Infasurf® improved lung mechanics more than Survanta® (top panel), and the importance of SP-B in this behavior is shown by the increased activity of Survanta® + SP-B compared to Survanta® alone (bottom panel). Surfactants were instilled intratracheally at a dose of 100 mg/kg body weight, and quasistatic P-V curves were measured following 15 min of mechanical ventilation. Data are redrawn from Mizuno et al [175].
References
-
- Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, et al. The American-European Consensus Conference on ARDS: Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994;149:818–824. - PubMed
-
- Murray JF, Matthay MA, Luce JM, Flick MR. An expanded definition of the adult respiratory distress syndrome. Am Rev Respir Dis. 1988;138:720–723. - PubMed
-
- American College of Chest Physicians Society of Critical Care Medicine Consensus Conference Committee. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies for sepsis; Crit Care Med; 1992. pp. 864–874. - PubMed
-
- Pollack MM, Patel KM, Ruttimann UE. PRISM III: An updated pediatric risk of mortality score. Crit Care Med. 1996;24:743–752. - PubMed
-
- Slater A, Shann F. ANZICS Paediatric Study Group. The suitability of the Pediatric Index of Mortality (PIM), PIM2, the Pediatric Risk of Mortality (PRISM), and PRISM III for monitoring the quality of pediatric intensive care in Australia and New Zealand. Pediatr Crit Care Med. 2004;5:447–454. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
