

Cardiovascular disease risk in type 2 diabetes mellitus: insights from mechanistic studies
- PMID: 18502305
- PMCID: PMC2774464
- DOI: 10.1016/S0140-6736(08)60768-0
Cardiovascular disease risk in type 2 diabetes mellitus: insights from mechanistic studies
Abstract
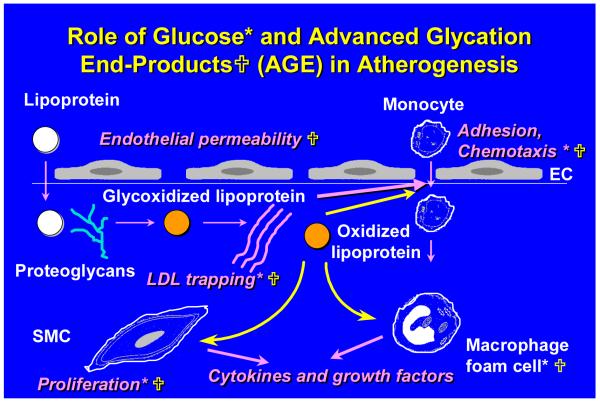
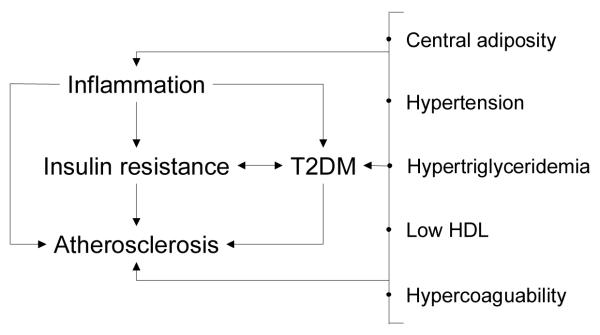
Individuals with type 2 diabetes mellitus have increased cardiovascular disease risk compared with those without diabetes. Treatment of the residual risk, other than blood pressure and LDL-cholesterol control, remains important as the rate of diabetes increases worldwide. The accelerated atherosclerosis and cardiovascular disease in diabetes is likely to be multifactorial and therefore several therapeutic approaches can be considered. Results of mechanistic studies done in vitro and in vivo--animals and people--can provide important insights with the potential to improve clinical management decisions and outcomes. In this Review, we focus on three areas in which pathophysiological considerations could be particularly informative--ie, the roles of hyperglycaemia, diabetic dyslipidaemia (other than the control of LDL-cholesterol concentrations), and inflammation (including that in adipose tissue) in the acceleration of vascular injury.
Figures
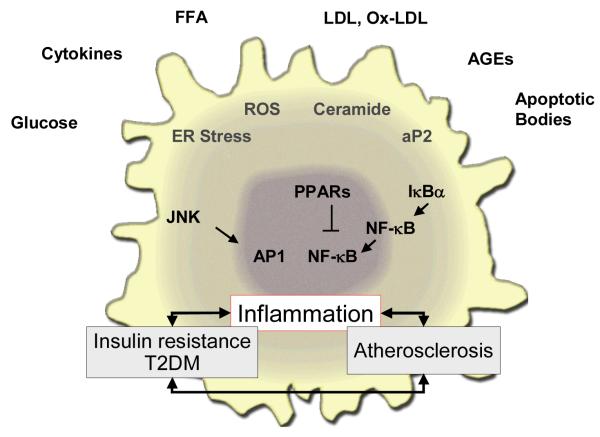
 ) have been shown to affect various steps in these pathways as shown.
) have been shown to affect various steps in these pathways as shown.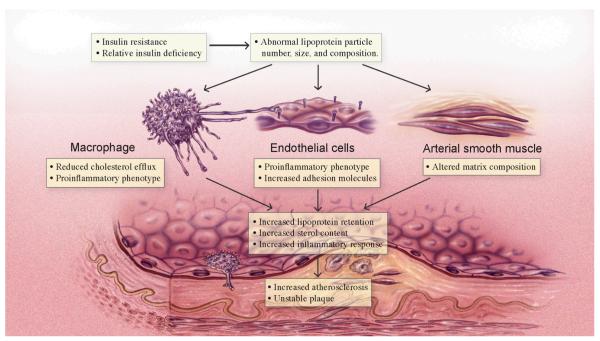
References
-
- Balkau B, Hu G, Qiao Q, Tuomilehto J, Borch-Johnsen K, Pyorala K. Prediction of the risk of cardiovascular mortality using a score that includes glucose as a risk factor: The DECODE Study. Diabetologia. 2004;47:2118–28. - PubMed
-
- UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glucose control with sulphonylureas or insluin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet. 1998;352:837–53. - PubMed
-
- For Safety, NHLBI Changes Intensive Blood Sugar Treatment Strategy in Clinical Trial of Diabetes and Cardiovascular Disease [news release] National Heart, Lung, and Blood Institute Communication Office; [Accessed March 7, 2006]. http://public.nhlbi.nih.gov/newsroom/home/GetPressRelease.aspx?id=2551. 2-3-2006. Ref Type: Internet Communication.
-
- ADVANCE Management Committee Study rationale and design of ADVANCE: action in diabetes and vascular disease-preterax and diamicron MR controlled evaluation. Diabetologia. 2008;44:1118–20. - PubMed
-
- Piga R, Naito Y, Kokura S, Handa O, Yoshikawa T. Short-term high glucose exposure induces monocyte-endothelial cells adhesion and transmigration by increasing VCAM-1 and MCP-1 expression in human aortic endothelial cells. Atherosclerosis. 2007;193:328–34. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P01 HL018645/HL/NHLBI NIH HHS/United States
- P01 HL030086/HL/NHLBI NIH HHS/United States
- P01 HL048743/HL/NHLBI NIH HHS/United States
- R01 HL039653/HL/NHLBI NIH HHS/United States
- HL071745/HL/NHLBI NIH HHS/United States
- DK71711/DK/NIDDK NIH HHS/United States
- HL30086/HL/NHLBI NIH HHS/United States
- HL19645/HL/NHLBI NIH HHS/United States
- R01 HL071745/HL/NHLBI NIH HHS/United States
- R01 DK071711/DK/NIDDK NIH HHS/United States
- R56 DK071711/DK/NIDDK NIH HHS/United States
- HL39653/HL/NHLBI NIH HHS/United States
- HL48743/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
