

Prone positioning and acute respiratory distress syndrome after cardiac surgery: a feasibility study
- PMID: 18503930
- PMCID: PMC9941421
- DOI: 10.1053/j.jvca.2007.10.013
Prone positioning and acute respiratory distress syndrome after cardiac surgery: a feasibility study
Abstract
Objective: To determine the feasibility, safety, and efficacy on PaO(2)/F(I)O(2) ratio of prone positioning (PP) for acute respiratory distress syndrome (ARDS) after cardiac surgery.
Design: Retrospective review of information entered prospectively in the authors' database.
Setting: A private community nonteaching hospital.
Participants: Sixteen patients who developed ARDS after cardiac surgery from January 2004 through June 2005.
Interventions: PP to improve oxygenation.
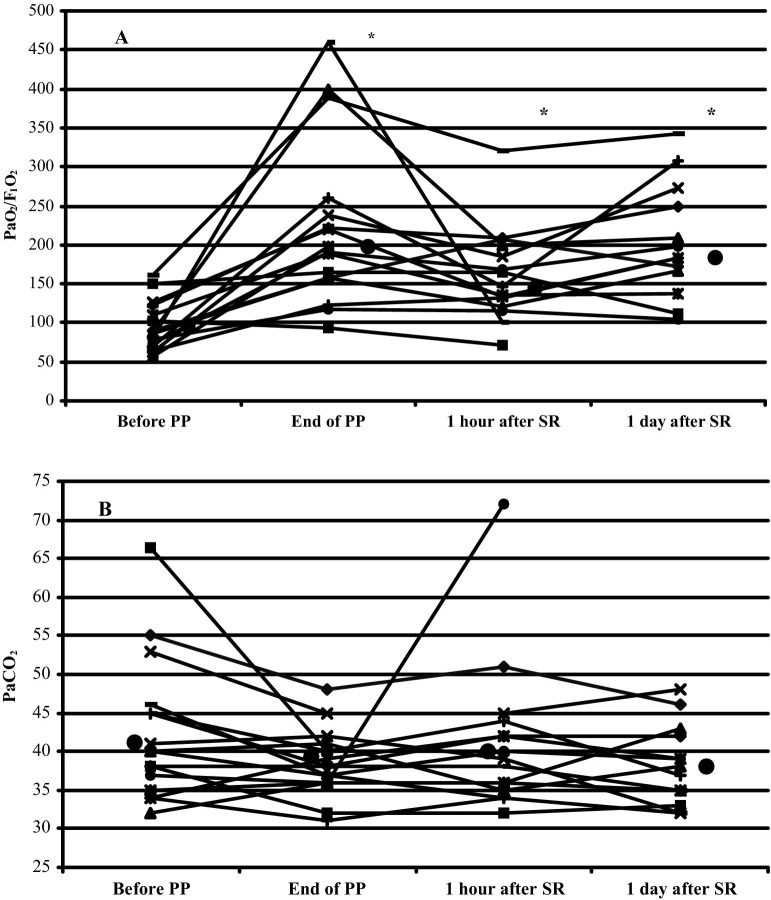
Measurements and main results: After a median duration of 18 (range, 14-27) hours in PP, PaO(2)/F(I)O(2) improved in 14 (87.5%) patients. For the entire population, median PaO(2)/F(I)O(2) rose from 87 (range, 56-161) before PP to 194 (range, 94-460; p < 0.05) after it. After supine repositioning (SR), PaO(2)/F(I)O(2) declined to 146 (range, 72-320; not significant). PaO(2)/F(I)O(2) at the end of PP and 1 day after SR were comparable, respectively, 194 (range, 94-460) and 184 (range, 105-342). No severe complication was associated with PP, but 5 patients developed pressure sores and 2 others had superficial sternal wound infections. Intensive care unit mortality of 37.5% reflected the number of organ failure(s); there were no deaths with 2 failures, and 60% with > or = 3 organ failures died (p = 0.03). Mortality rates were comparable regardless of whether patients were PaO(2)/F(I)O(2) responders or their PaCO(2) decreased by > or = 1 mmHg.
Conclusion: PP to treat ARDS after cardiac surgery is feasible, safe, and can efficiently improve oxygenation. Measures to prevent pressure sores are mandatory.
Figures
References
-
- Asimakopoulos G., Taylor K.M., Smith P.L., et al. Prevalence of acute respiratory distress syndrome after cardiac surgery. J Thorac Cardiovasc Surg. 1999;117:620–621. - PubMed
-
- Kaul T.K., Fields B.L., Riggins L.S., et al. Adult respiratory distress syndrome following cardiopulmonary bypass: Incidence, prophylaxis and management. J Cardiovasc Surg. 1998;39:777–781. - PubMed
-
- Milot J., Perron J., Lacasse Y., et al. Incidence and predictors of ARDS after cardiac surgery. Chest. 2001;119:884–888. - PubMed
-
- Messent M., Sullivan K., Keogh B.F., et al. Adult respiratory distress syndrome following cardiopulmonary bypass: Incidence and prediction. Anaesthesia. 1992;47:267–268. - PubMed
-
- Christenson J.T., Aeberhard J.M., Badel P., et al. Adult respiratory distress syndrome after cardiac surgery. Cardiovasc Surg. 1996;4:15–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
