

Weight loss alone improves conduit and resistance artery endothelial function in young and older overweight/obese adults
- PMID: 18504322
- PMCID: PMC2913284
- DOI: 10.1161/HYPERTENSIONAHA.108.111427
Weight loss alone improves conduit and resistance artery endothelial function in young and older overweight/obese adults
Abstract
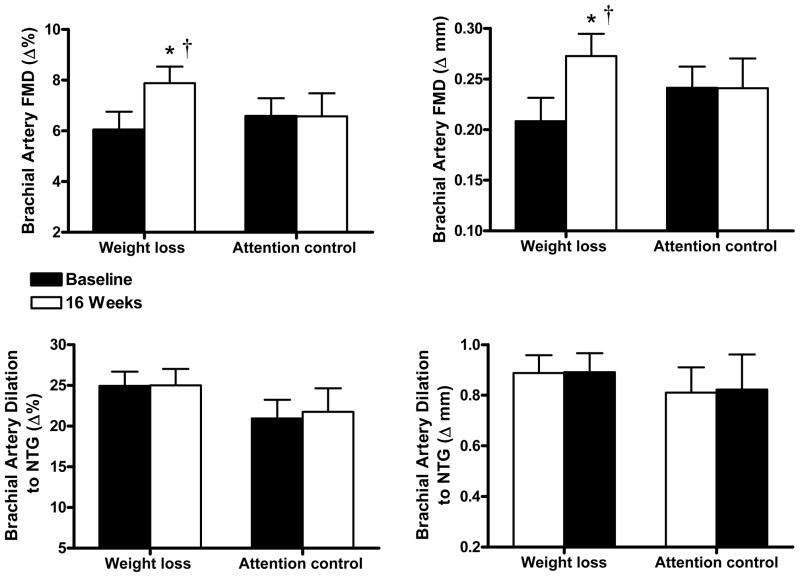
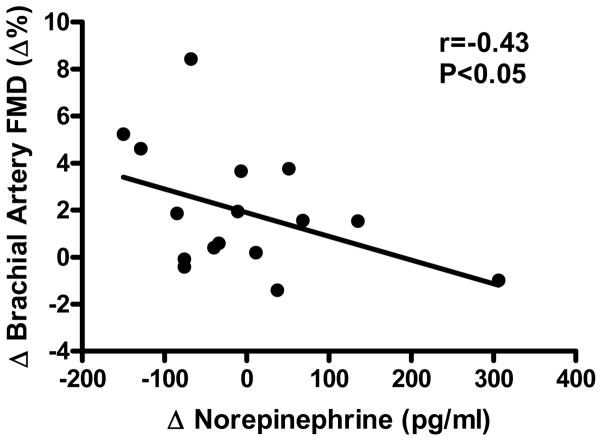
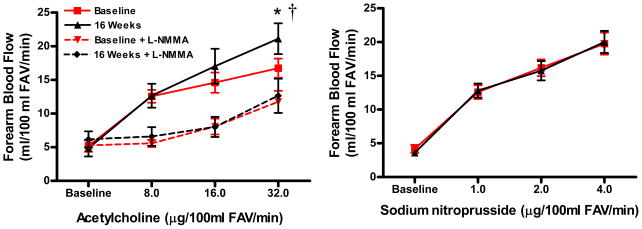
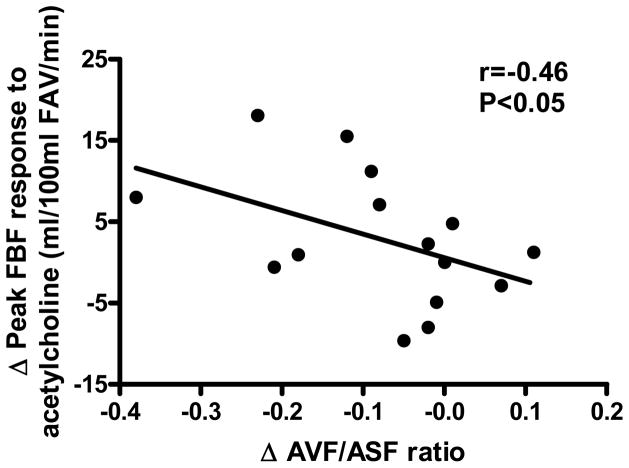
Obesity is associated with vascular endothelial dysfunction, as indicated by impaired endothelium-dependent dilation. Presently there is no direct evidence that energy intake-restricted weight loss alone improves conduit or resistance artery endothelium-dependent dilation, the mechanisms involved, or whether improvements differ with patient age. A total of 40 overweight or obese (body mass index: >or=25<40 kg/m(2)) nondiabetic men and women aged 21 to 69 years completed 12 weeks of reduced energy intake (n=26; 15 male) or attention control (n=14; 9 male) and 4 weeks of weight maintenance (randomized trial). Energy intake restriction reduced estimated total energy intake (33%), body weight (10.5%), total and abdominal body fat, plasma leptin, oxidized low-density lipoprotein, and improved several metabolic risk factors. Brachial artery flow-mediated dilation was increased by 30% (6.0+/-0.7% versus 7.9+/-0.7%Delta; P=0.01; n=17). Peak forearm blood flow during intrabrachial artery infusion of acetylcholine was increased by 26% (16.8+/-1.4 versus 21.1+/-1.9 mL/100 mL per minute; P<0.05; n=15); this was inversely related to the reduction in the abdominal visceral:subcutaneous fat ratio (r=-0.46; P<0.05) and was abolished by inhibition of NO synthesis with N(G)-monomethyl-L-arginine. Improvements in endothelium-dependent dilation were not related to age: mean increases in subjects >50 years of age were similar to or greater than those <50 years of age. Energy intake-restricted weight loss alone is an effective intervention for improving peripheral conduit and resistance artery endothelial function in young and older overweight/obese adults. The improvements in resistance artery function are mediated by an increase in NO bioavailability and are related to reductions in abdominal visceral fat.
Figures
Comment in
-
Weight loss and vascular function: the good and the unknown.Hypertension. 2008 Jul;52(1):57-8. doi: 10.1161/HYPERTENSIONAHA.108.112441. Epub 2008 May 26. Hypertension. 2008. PMID: 18504320 No abstract available.
References
-
- Williams I, Wheatcroft S, Shah A, Kearny M. Obesity, atherosclerosis and the vascular endothelium: mechanisms of reduced nitric oxide bioavailability in obese humans. Int J Obes. 2002;26:754–764. - PubMed
-
- Brook RD. Obesity, weight loss, and vascular function. Endocrine. 2006;29(1):21–25. - PubMed
-
- Yeboah J, Crouse JR, Hsu FC, Burke GL, Herrington DM. Brachial flow-mediated dilation predicts incident cardiovascular events in older adults: the Cardiovascular Health Study. Circulation. 2007;115:2390–2397. - PubMed
-
- Gokce N, Keaney JF, Jr, Hunter LM, Watkins MT, Nedeljkovic ZS, Menzoian JO, Vita JA. Predictive value of noninvasively determined endothelial dysfunction for long-term cardiovascular events in patients with peripheral vascular disease. J Am Coll Cardiol. 2003;41:1769–1775. - PubMed
