

Natural history of asymptomatic patients with normally functioning or minimally dysfunctional bicuspid aortic valve in the community
- PMID: 18506017
- PMCID: PMC2878133
- DOI: 10.1161/CIRCULATIONAHA.107.740878
Natural history of asymptomatic patients with normally functioning or minimally dysfunctional bicuspid aortic valve in the community
Abstract
Background: Bicuspid aortic valve is frequent and is reported to cause numerous complications, but the clinical outcome of patients diagnosed with normal or mildly dysfunctional valve is undefined.
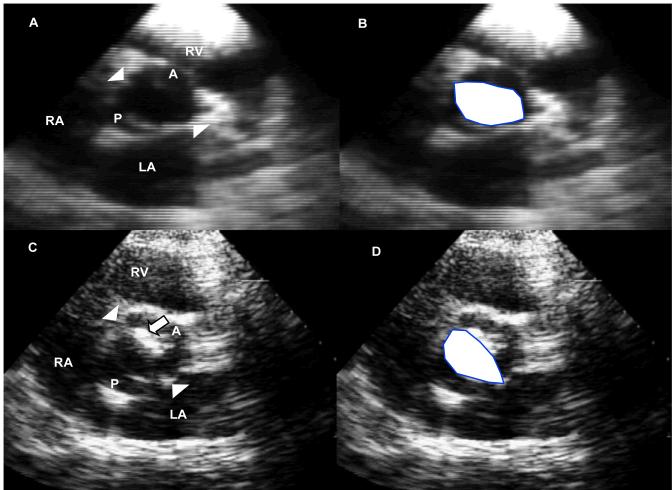
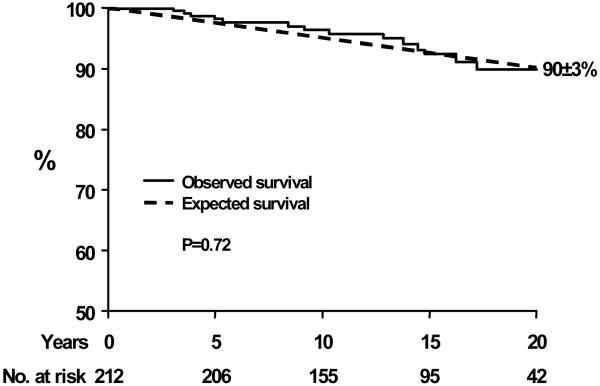
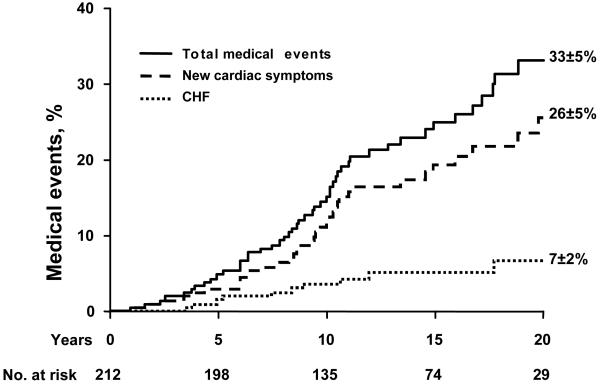
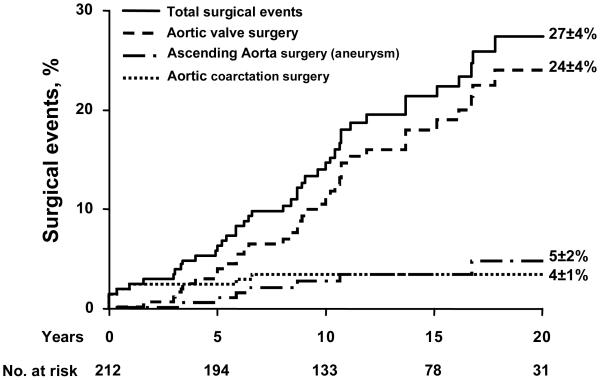
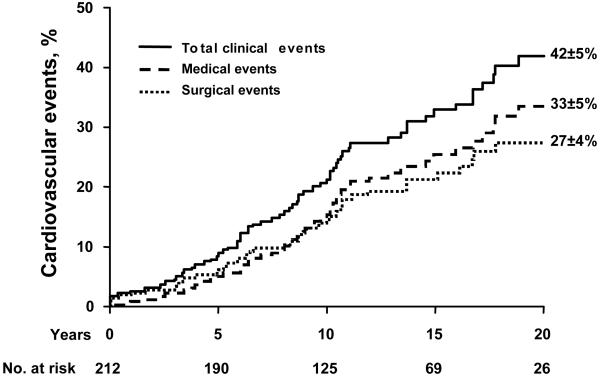
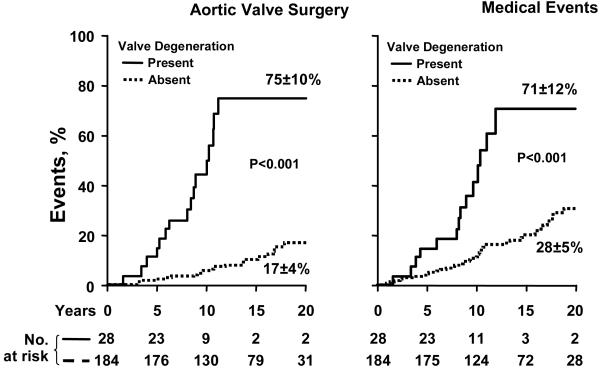
Methods and results: In 212 asymptomatic community residents from Olmsted County, Minn (age, 32+/-20 years; 65% male), bicuspid aortic valve was diagnosed between 1980 and 1999 with ejection fraction > or =50% and aortic regurgitation or stenosis, absent or mild. Aortic valve degeneration at diagnosis was scored echocardiographically for calcification, thickening, and mobility reduction (0 to 3 each), with scores ranging from 0 to 9. At diagnosis, ejection fraction was 63+/-5% and left ventricular diameter was 48+/-9 mm. Survival 20 years after diagnosis was 90+/-3%, identical to the general population (P=0.72). Twenty years after diagnosis, heart failure, new cardiac symptoms, and cardiovascular medical events occurred in 7+/-2%, 26+/-4%, and 33+/-5%, respectively. Twenty years after diagnosis, aortic valve surgery, ascending aortic surgery, or any cardiovascular surgery was required in 24+/-4%, 5+/-2%, and 27+/-4% at a younger age than the general population (P<0.0001). No aortic dissection occurred. Thus, cardiovascular medical or surgical events occurred in 42+/-5% 20 years after diagnosis. Independent predictors of cardiovascular events were age > or =50 years (risk ratio, 3.0; 95% confidence interval, 1.5 to 5.7; P<0.01) and valve degeneration at diagnosis (risk ratio, 2.4; 95% confidence interval, 1.2 to 4.5; P=0.016; >70% events at 20 years). Baseline ascending aorta > or =40 mm independently predicted surgery for aorta dilatation (risk ratio, 10.8; 95% confidence interval, 1.8 to 77.3; P<0.01).
Conclusions: In the community, asymptomatic patients with bicuspid aortic valve and no or minimal hemodynamic abnormality enjoy excellent long-term survival but incur frequent cardiovascular events, particularly with progressive valve dysfunction. Echocardiographic valve degeneration at diagnosis separates higher-risk patients who require regular assessment from lower-risk patients who require only episodic follow-up.
Figures
References
-
- Roberts WC. The congenitally bicuspid aortic valve. A study of 85 autopsy cases. Am J Cardiol. 1970;26:72–83. - PubMed
-
- Larson EW, Edwards WD. Risk factors for aortic dissection: a necropsy study of 161 cases. Am J Cardiol. 1984;53:849–55. - PubMed
-
- Steinberger J, Moller JH, Berry JM, Sinaiko AR. Echocardiographic diagnosis of heart disease in apparently healthy adolescents. Pediatrics. 2000;105:815–8. - PubMed
-
- Lamas CC, Eykyn SJ. Bicuspid aortic valve--A silent danger: analysis of 50 cases of infective endocarditis. Clin Infect Dis. 2000;30:336–41. - PubMed
-
- Fenoglio JJ, Jr., McAllister HA, Jr., DeCastro CM, Davia JE, Cheitlin MD. Congenital bicuspid aortic valve after age 20. Am J Cardiol. 1977;39:164–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
