

HLA sensitization and allograft bone graft incorporation
- PMID: 18506564
- PMCID: PMC2584269
- DOI: 10.1007/s11999-008-0294-4
HLA sensitization and allograft bone graft incorporation
Abstract
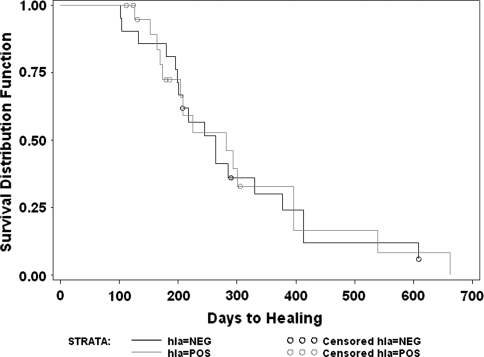
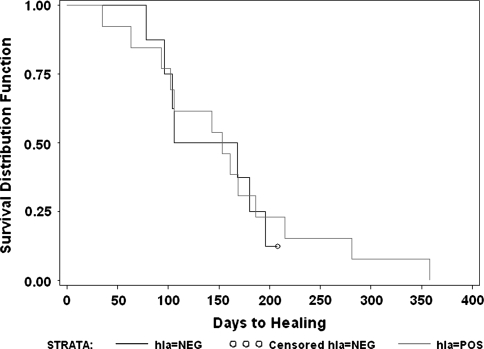
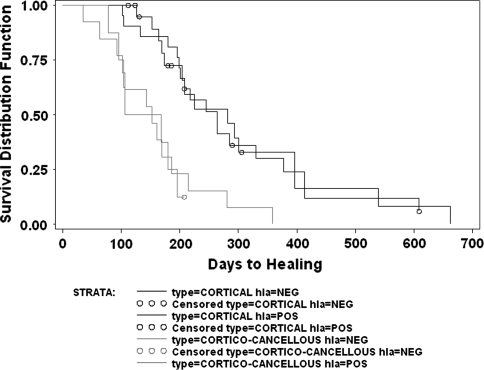
Achieving union between host bone and massive structural allografts can be difficult. Donor and recipient human leukocyte antigen (HLA) mismatches and recipient antibody response to donor HLA antigens might affect union. In a prospective multiinstitutional study, we enrolled a consecutive series of patients receiving cortex-replacing, massive structural bone allografts to determine the rate of donor-specific HLA antibody sensitization and to investigate the potential effect of such HLA alloantibody sensitization on allograft incorporation. HLA typing of patients and donors was determined by molecular typing methods. Donor-specific HLA sensitization occurred in 57% of the patients but had no demonstrable effect on graft incorporation or union. The type of host-allograft junction did have a major effect on graft incorporation. Cortical-to-cortical allograft-to-host junctions healed more slowly (mean, 542 days) than corticocancellous to corticocancellous allograft-to-host junctions (mean, 243 days). Although HLA sensitization does not appear to delay structural allograft bone incorporation, further followup is required to determine if there is an association between HLA sensitization and long-term graft survival. Based on these preliminary data, measures to further minimize or modulate HLA sensitization or response are not indicated at present for the purposes of improving structural bone allograft union.
Level of evidence: Level II, prognostic study.
Figures








Similar articles
-
Human leukocyte antigen sensitization after structural cortical allograft implantations.Clin Orthop Relat Res. 2005 Jun;(435):31-5. doi: 10.1097/01.blo.0000165848.43820.98. Clin Orthop Relat Res. 2005. PMID: 15930918
-
Donor-Specific Human Leukocyte Antigen Antibody Formation After Allograft Glenoid Reconstruction Occurs But Does Not Impact Clinicoradiographic Outcomes.Am J Sports Med. 2021 Apr;49(5):1175-1182. doi: 10.1177/0363546521996701. Epub 2021 Mar 5. Am J Sports Med. 2021. PMID: 33667132 Free PMC article.
-
Aortic valve allograft structural deterioration is associated with a subset of antibodies to human leukocyte antigens.J Heart Valve Dis. 2003 May;12(3):382-90; discussion 390-1. J Heart Valve Dis. 2003. PMID: 12803340
-
Humoral Immune Response and Allograft Function in Kidney Transplantation.Am J Kidney Dis. 2015 Aug;66(2):337-47. doi: 10.1053/j.ajkd.2015.03.033. Epub 2015 May 16. Am J Kidney Dis. 2015. PMID: 25987262 Review.
-
Do allografts present a risk to burn patients? Allografts and HLA-sensitization.Burns. 2025 May;51(4):107424. doi: 10.1016/j.burns.2025.107424. Epub 2025 Feb 14. Burns. 2025. PMID: 40121705
Cited by
-
Characterization of immunologically detectable T-cell sensitization, Immunohistochemical detection of pro-inflammatory cytokines, and clinical parameters of patients after allogeneic intraoral bone grafting procedures: a prospective randomized controlled clinical trial in humans.BMC Oral Health. 2022 Dec 10;22(1):592. doi: 10.1186/s12903-022-02584-6. BMC Oral Health. 2022. PMID: 36496367 Free PMC article. Clinical Trial.
-
Characterization of circulating DNA in plasma of patients after allogeneic bone grafting.Clin Oral Investig. 2019 Dec;23(12):4243-4253. doi: 10.1007/s00784-019-02867-3. Epub 2019 Mar 3. Clin Oral Investig. 2019. PMID: 30826920
-
Osteoimmunology: Interactions With the Immune System in Spinal Fusion.Int J Spine Surg. 2023 Dec 27;17(S3):S9-S17. doi: 10.14444/8556. Int J Spine Surg. 2023. PMID: 38050073 Free PMC article.
-
Comparative Analysis of Heavy Metal Content in Impacted Third Molars from Industrial and Non-Industrial Areas and Its Effect on the Isolation, Culture, and Proliferation of Dental Stem Cells (DSCs).J Clin Med. 2024 Sep 14;13(18):5465. doi: 10.3390/jcm13185465. J Clin Med. 2024. PMID: 39336954 Free PMC article.
-
Preliminary outcomes of allograft and hydroxyapatite as substitutes for autograft in anterior cervical discectomy and fusion with self-locking standalone cages.J Orthop Surg Res. 2021 Feb 8;16(1):123. doi: 10.1186/s13018-021-02257-0. J Orthop Surg Res. 2021. PMID: 33557893 Free PMC article.
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '9577428', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/9577428/'}]}
- Aho AJ, Eskola J, Ekfors T, Manner I, Kouri T, Hollmen T. Immune responses and clinical outcome of massive human osteoarticular allografts. Clin Orthop Relat Res. 1997;346:196–206. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '3416079', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/3416079/'}]}
- Andrew G, Dewailly J, Leberre C, Quarre MC, Bidet ML, Tardivel R, Devers L, Lam Y, Soreau E, Boccaccio C. Prevention of HLA immunization with leukocyte-poor packed red cells and platelet concentrates obtained by filtration. Blood. 1988;72:964–969. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.3109/07853899309147303', 'is_inner': False, 'url': 'https://doi.org/10.3109/07853899309147303'}, {'type': 'PubMed', 'value': '8217107', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/8217107/'}]}
- Aro HT, Aho AJ. Clinical use of bone allografts. Ann Med. 1993;25:403–412. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '6336761', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/6336761/'}]}
- Bos GD, Goldberg VM, Powell AE, Heiple KG, Zika JM. The effect of histocompatibility matching on canine frozen bone allografts. J Bone Joint Surg Am. 1983;65:89–96. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '349741', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/349741/'}]}
- Burchardt H, Enneking WF. Transplantation of bone. Surg Clin North Am. 1978;58:403–427. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
