

Endogenous sex hormones and endometrial cancer risk in women in the European Prospective Investigation into Cancer and Nutrition (EPIC)
- PMID: 18509001
- PMCID: PMC2396334
- DOI: 10.1677/ERC-07-0064
Endogenous sex hormones and endometrial cancer risk in women in the European Prospective Investigation into Cancer and Nutrition (EPIC)
Abstract
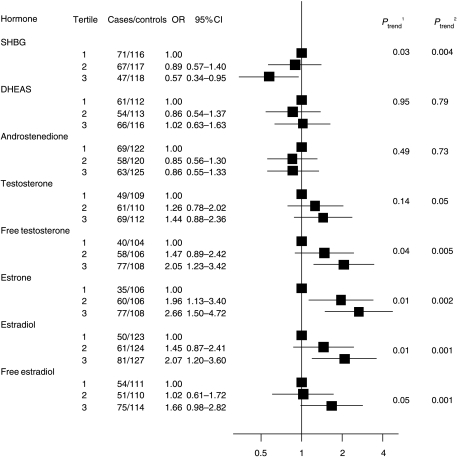
Epidemiological data show that reproductive and hormonal factors are involved in the etiology of endometrial cancer, but there is little data on the association with endogenous sex hormone levels. We analyzed the association between prediagnostic serum concentrations of sex steroids and endometrial cancer risk in the European Prospective Investigation into Cancer and Nutrition using a nested case-control design of 247 incident endometrial cancer cases and 481 controls, matched on center, menopausal status, age, variables relating to blood collection, and, for premenopausal women, phase of menstrual cycle. Using conditional regression analysis, endometrial cancer risk among postmenopausal women was positively associated with increasing levels of total testosterone, free testosterone, estrone, total estradiol, and free estradiol. The odds ratios (ORs) for the highest versus lowest tertile were 2.66 (95% confidence interval (CI) 1.50-4.72; P=0.002 for a continuous linear trend) for estrone, 2.07 (95% CI 1.20-3.60; P=0.001) for estradiol, and 1.66 (95% CI 0.98-2.82; P=0.001) for free estradiol. For total and free testosterone, ORs for the highest versus lowest tertile were 1.44 (95% CI 0.88-2.36; P=0.05) and 2.05 (95% CI 1.23-3.42; P=0.005) respectively. Androstenedione and dehydroepiandrosterone sulfate were not associated with risk. Sex hormone-binding globulin was significantly inversely associated with risk (OR for the highest versus lowest tertile was 0.57, 95% CI 0.34-0.95; P=0.004). In premenopausal women, serum sex hormone concentrations were not clearly associated with endometrial cancer risk, but numbers were too small to draw firm conclusions. In conclusion, relatively high blood concentrations of estrogens and free testosterone are associated with an increased endometrial cancer risk in postmenopausal women.
Figures

References
-
- Austin H, Austin JM, Jr, Partridge EE, Hatch KD, Shingleton HM. Endometrial cancer, obesity, and body fat distribution. Cancer Research. 1991;51:568–572. - PubMed
-
- Baanders-van Halewijn EA, Poortman J. A case–control study of endometrial cancer within a cohort. Maturitas. 1985;7:69–76. - PubMed
-
- Beral V, Bull D, Reeves G. Endometrial cancer and hormone-replacement therapy in the Million Women Study. Lancet. 2005;365:1543–1551. - PubMed
-
- Bergstrom A, Pisani P, Tenet V, Wolk A, Adami HO. Overweight as an avoidable cause of cancer in Europe. International Journal of Cancer. 2001;91:421–430. - PubMed
-
- Bray F, Loos AH, Oostindier M, Weiderpass E. Geographic and temporal variations in cancer of the corpus uteri: incidence and mortality in pre- and postmenopausal women in Europe. International Journal of Cancer. 2005;117:123–131. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
