

A systematic review with procedural assessments and meta-analysis of low level laser therapy in lateral elbow tendinopathy (tennis elbow)
- PMID: 18510742
- PMCID: PMC2442599
- DOI: 10.1186/1471-2474-9-75
A systematic review with procedural assessments and meta-analysis of low level laser therapy in lateral elbow tendinopathy (tennis elbow)
Abstract
Background: Recent reviews have indicated that low level level laser therapy (LLLT) is ineffective in lateral elbow tendinopathy (LET) without assessing validity of treatment procedures and doses or the influence of prior steroid injections.
Methods: Systematic review with meta-analysis, with primary outcome measures of pain relief and/or global improvement and subgroup analyses of methodological quality, wavelengths and treatment procedures.
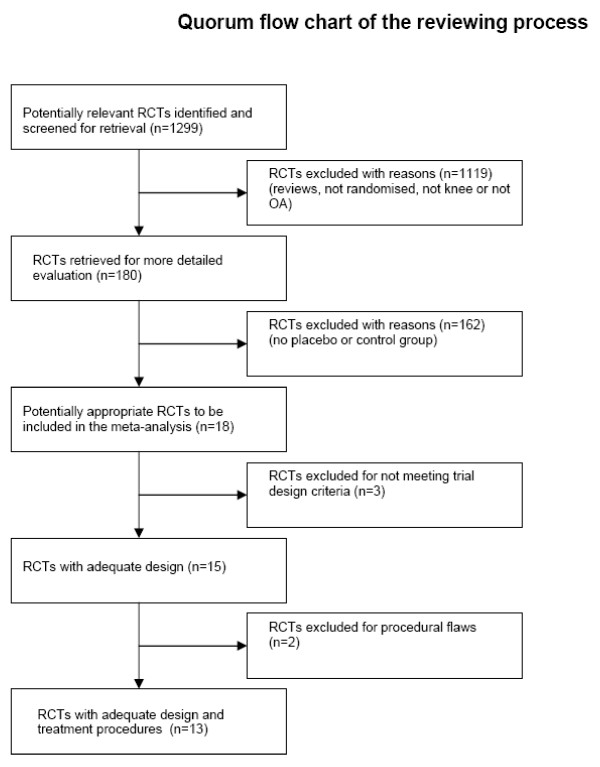
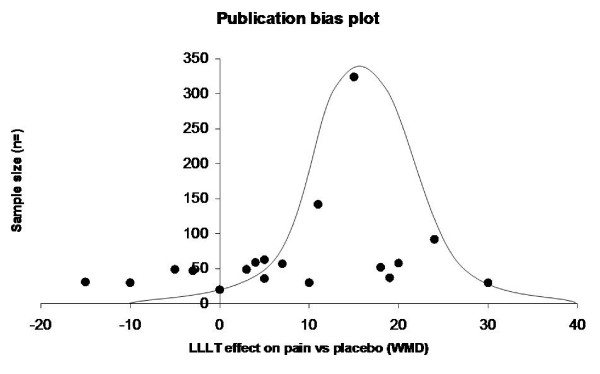
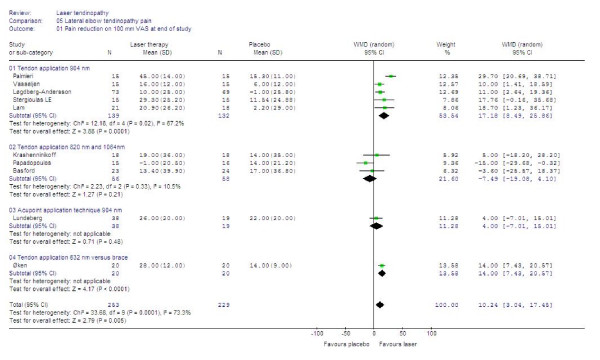
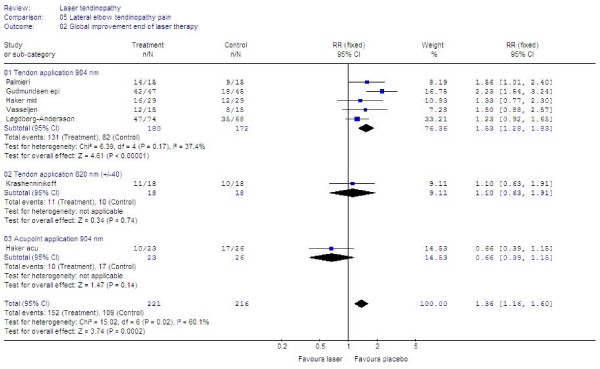
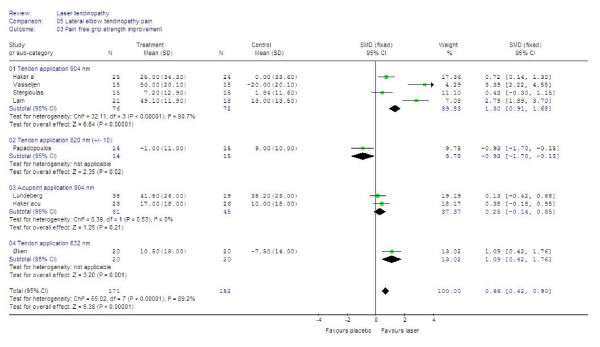
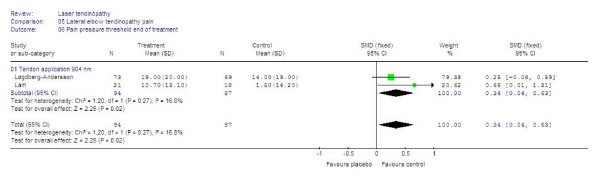
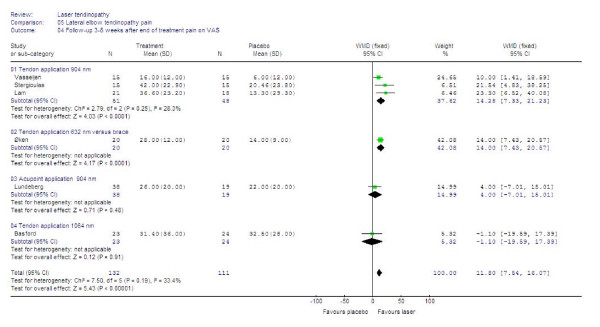
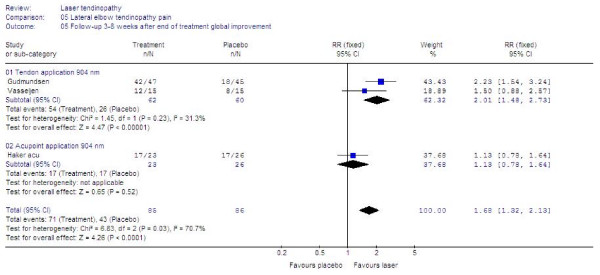
Results: 18 randomised placebo-controlled trials (RCTs) were identified with 13 RCTs (730 patients) meeting the criteria for meta-analysis. 12 RCTs satisfied half or more of the methodological criteria. Publication bias was detected by Egger's graphical test, which showed a negative direction of bias. Ten of the trials included patients with poor prognosis caused by failed steroid injections or other treatment failures, or long symptom duration or severe baseline pain. The weighted mean difference (WMD) for pain relief was 10.2 mm [95% CI: 3.0 to 17.5] and the RR for global improvement was 1.36 [1.16 to 1.60]. Trials which targeted acupuncture points reported negative results, as did trials with wavelengths 820, 830 and 1064 nm. In a subgroup of five trials with 904 nm lasers and one trial with 632 nm wavelength where the lateral elbow tendon insertions were directly irradiated, WMD for pain relief was 17.2 mm [95% CI: 8.5 to 25.9] and 14.0 mm [95% CI: 7.4 to 20.6] respectively, while RR for global pain improvement was only reported for 904 nm at 1.53 [95% CI: 1.28 to 1.83]. LLLT doses in this subgroup ranged between 0.5 and 7.2 Joules. Secondary outcome measures of painfree grip strength, pain pressure threshold, sick leave and follow-up data from 3 to 8 weeks after the end of treatment, showed consistently significant results in favour of the same LLLT subgroup (p < 0.02). No serious side-effects were reported.
Conclusion: LLLT administered with optimal doses of 904 nm and possibly 632 nm wavelengths directly to the lateral elbow tendon insertions, seem to offer short-term pain relief and less disability in LET, both alone and in conjunction with an exercise regimen. This finding contradicts the conclusions of previous reviews which failed to assess treatment procedures, wavelengths and optimal doses.
Figures
References
-
- Smidt N, Lewis M, DA VDW, Hay EM, Bouter LM, Croft P. Lateral epicondylitis in general practice: course and prognostic indicators of outcome. J Rheumatol. 2006;33:2053–59. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
