

Monosomy 1p36 uncovers a role for OX40 in survival of activated CD4+ T cells
- PMID: 18511345
- PMCID: PMC2583253
- DOI: 10.1016/j.clim.2008.03.522
Monosomy 1p36 uncovers a role for OX40 in survival of activated CD4+ T cells
Abstract
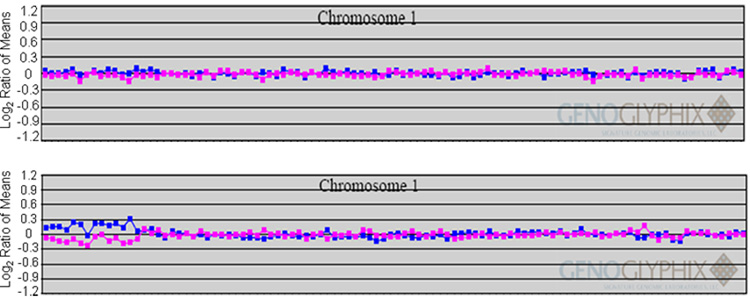
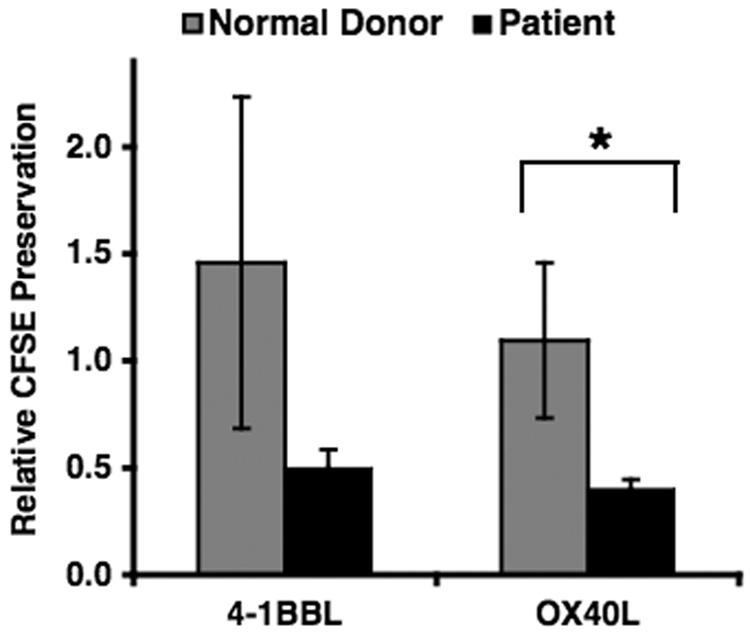
Monosomy 1p36 is a subtelomeric deletion syndrome associated with congenital anomalies presumably due to haploinsufficiency of multiple genes. Although immunodeficiency has not been reported, genes encoding costimulatory molecules of the TNF receptor superfamily (TNFRSF) are within 1p36 and may be affected. In one patient with monosomy 1p36, comparative genome hybridization and fluorescence in- situ hybridization confirmed that TNFRSF member OX40 was included within the subtelomeric deletion. T cells from this patient had decreased OX40 expression after stimulation. Specific, ex vivo T cell activation through OX40 revealed enhanced proliferation, and reduced viability of patient CD4+ T cells, providing evidence for the association of monosomy 1p36 with reduced OX40 expression, and decreased OX40-induced T cell survival. These results support a role for OX40 in human immunity, and calls attention to the potential for haploinsufficiency deletions of TNFRSF costimulatory molecules in monosomy 1p36.
Figures






References
-
- Kurosawa K, Kawame H, Okamoto N, Ochiai Y, Akatsuka A, Kobayashi M, Shimohira M, Mizuno S, Wada K, Fukushima Y, Kawawaki H, Yamamoto T, Masuno M, Imaizumi K, Kuroki Y. Epilepsy and neurological findings in 11 individuals with 1p36 deletion syndrome. Brain & Development. 2005;27:378–382. - PubMed
-
- Gajecka M, Yu W, Ballif BC, Glotzbach CD, Bailey KA, Shaw CA, Kashork CD, Heilstedt HA, Ansel DA, Theisen A, Rice R, Rice DPC, Shaffer LG. Delineation of mechanisms and regions of dosage imbalance in complex rearrangements of 1p36 leads to a putative gene for regulation of cranial suture closure. European Journal of Human Genetics. 2005;13:139–149. - PubMed
-
- Neumann LM, Polster T, Spantzel T, Bartsch O. Unexpected death of a 12 year old boy with monosomy 1p36. Genetic Counseling. 2004;15:19–26. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
