

Vascular access use and outcomes: an international perspective from the Dialysis Outcomes and Practice Patterns Study
- PMID: 18511606
- PMCID: PMC2542410
- DOI: 10.1093/ndt/gfn261
Vascular access use and outcomes: an international perspective from the Dialysis Outcomes and Practice Patterns Study
Erratum in
- Nephrol Dial Transplant. 2008 Dec;23(12):4088
Abstract
Background: A well-functioning vascular access (VA) is essential to efficient dialysis therapy. Guidelines have been implemented improving care, yet access use varies widely across countries and VA complications remain a problem. This study took advantage of the unique opportunity to utilize data from the Dialysis Outcomes and Practice Patterns Study (DOPPS) to examine international trends in VA use and trends in patient characteristics and practices associated with VA use from 1996 to 2007. DOPPS is a prospective, observational study of haemodialysis (HD) practices and patient outcomes at >300 HD units from 12 countries and has collected data thus far from >35,000 randomly selected patients.
Methods: VA data were collected for each patient at study entry (1996-2007). Practice pattern data from the facility medical director, nurse manager and VA surgeon were also analysed.
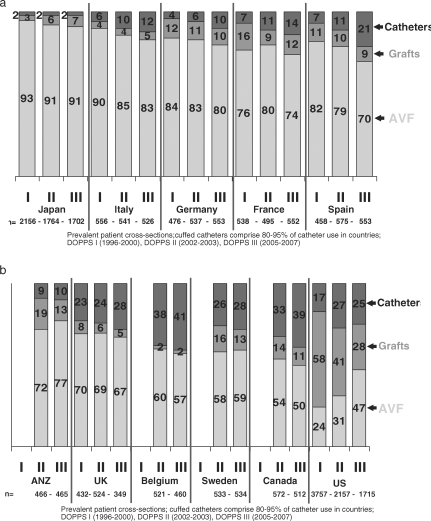
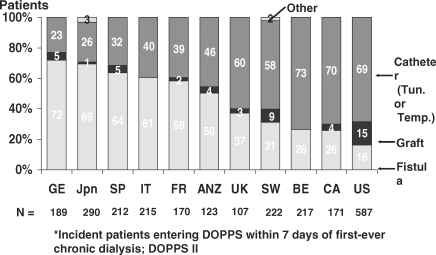
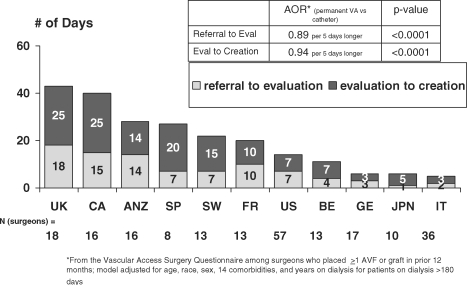
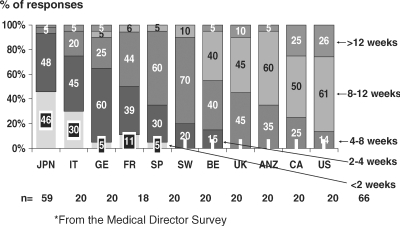
Results: Since 2005, a native arteriovenous fistula (AVF) was used by 67-91% of prevalent patients in Japan, Italy, Germany, France, Spain, the UK, Australia and New Zealand, and 50-59% in Belgium, Sweden and Canada. From 1996 to 2007, AVF use rose from 24% to 47% in the USA but declined in Italy, Germany and Spain. Moreover, graft use fell by 50% in the USA from 58% use in 1996 to 28% by 2007. Across three phases of data collection, patients consistently were less likely to use an AVF versus other VA types if female, of older age, having greater body mass index, diabetes, peripheral vascular disease or recurrent cellulitis/gangrene. In addition, countries with a greater prevalence of diabetes in HD patients had a significantly lower percentage of patients using an AVF. Despite poorer outcomes for central vein catheters, catheter use rose 1.5- to 3-fold among prevalent patients in many countries from 1996 to 2007, even among non-diabetic patients 18-70 years old. Furthermore, 58-73% of patients new to end-stage renal disease (ESRD) used a catheter for the initiation of HD in five countries despite 60-79% of patients having been seen by a nephrologist >4 months prior to ESRD. Patients were significantly (P < 0.05) less likely to start dialysis with a permanent VA if treated in a faciity that (1) had a longer time from referral to access surgery evaluation or from evaluation to access creation and (2) had longer time from access creation until first AVF cannulation. The median time from referral until access creation varied from 5-6 days in Italy, Japan and Germany to 40-43 days in the UK and Canada. Compared to patients using an AVF, patients with a catheter displayed significantly lower mean Kt/V levels.
Conclusions: Most countries meet the contemporary National Kidney Foundation's Kidney Disease Outcomes Quality Initiative goal for AVF use; however, there is still a wide variation in VA preference. Delays between the creation and cannulation must be improved to enhance the chances of a future permanent VA. Native arteriovenous fistula is the VA of choice ensuring dialysis adequacy and better patient outcomes. Graft is, however, a better alternative than catheter for patients where the creation of an attempted AVF failed or could not be created for different reasons.
Keywords: DOPPS; arteriovenous fistulae; catheter; haemodialysis; vascular access.
Figures
References
-
- Hoen B, Kessler M, Hestin D, et al. Risk factors for bacterial infections in chronic haemodialysis adult patients: a multicentre prospective survey. Nephrol Dial Transplant. 1995;10:377–381. - PubMed
-
- Combe C, Pisoni RL, Port FK, et al. Dialysis Outcomes and Practice Patterns Study: data on the use of central venous catheters in chronic hemodialysis. Néphrologie. 2001;22:379–384. - PubMed
-
- Feldman HI, Kobrin S, Wasserstein A. Hemodialysis vascular access morbidity. J Am Soc Nephrol. 1996;7:523–535. - PubMed
-
- Dixon BS, Novak L, Fangman J. Hemodialysis vascular access survival: upper-arm native arteriovenous fistula. Am J Kidney Dis. 2002;39:92–101. - PubMed
-
- Huber TS, Carter JW, Carter RL, et al. Patency of autogenous and polytetrafluoroethylene upper extremity arteriovenous hemodialysis accesses: a systematic review. J Vasc Surg. 2003;38:1005–1011. - PubMed
