

Vessel wall contrast enhancement: a diagnostic sign of cerebral vasculitis
- PMID: 18511868
- PMCID: PMC2813800
- DOI: 10.1159/000135649
Vessel wall contrast enhancement: a diagnostic sign of cerebral vasculitis
Abstract
Purpose: Inflammatory stenoses of cerebral arteries cause stroke in patients with florid vasculitis. However, diagnosis is often difficult even with digital subtraction angiography (DSA) and biopsy. The purpose of this study was to establish the value of contrast-enhanced MRI, proven to be sensitive to extradural arteritis, for the identification of intracranial vessel wall inflammation.
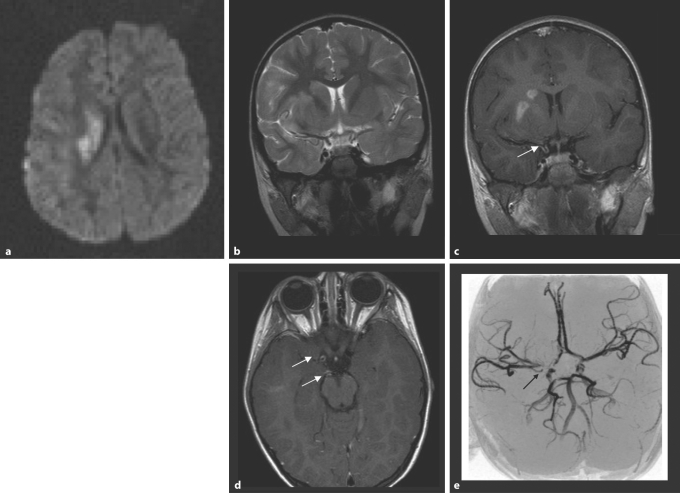
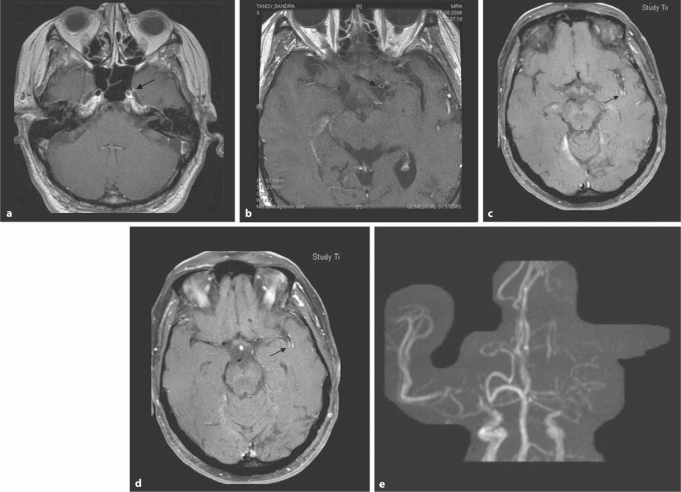
Patients and methods: Twenty-seven patients with a diagnosis of cerebral vasculitis affecting large brain vessels were retrieved from the files: 8 children (2-10 years, 7 female, 1 male) and 19 adults (16-76 years, 10 female, 9 male). Diagnosis was based on histological or serological proof of vasculitis or on clinical and imaging criteria. All MRI examinations included diffusion-weighted imaging, time-of-flight magnetic resonance angiography (TOF-MRA) and contrast-enhanced scans. MRI scans were assessed for the presence of ischemic brain lesions, arterial stenoses, vessel wall thickening and contrast uptake.
Results: Ischemic changes of the brain tissue were seen in 24/27 patients and restricted diffusion suggestive of recent ischemia in 17/27; 25/27 patients had uni- or multifocal stenoses of intracranial arteries on TOF-MRA and 5/6 had stenoses on DSA. Vessel wall thickening was identified in 25/27, wall enhancement in 23/27 patients.
Conclusion: Wall thickening and intramural contrast uptake are frequent findings in patients with active cerebral vasculitis affecting large brain arteries. Further prospective studies are required to determine the specificity of this finding.
(c) 2008 S. Karger AG, Basel
Figures
References
-
- Carvalho KS, Garg BP. Arterial strokes in children. Neurol Clin. 2002;20:1079–1100. vii. - PubMed
-
- Cerrato P, Grasso M, Imperiale D, Priano L, Baima C, Giraudo M, Rizzuto A, Azzaro C, Lentini A, Bergamasco B. Stroke in young patients: etiopathogenesis and risk factors in different age classes. Cerebrovasc Dis. 2004;18:154–159. - PubMed
-
- Benseler SM, Silverman E, Aviv RI, Schneider R, Armstrong D, Tyrrell PN, de Veber G. Primary central nervous system vasculitis in children. Arthritis Rheum. 2006;54:1291–1297. - PubMed
-
- Calabrese LH. Diagnostic strategies in vasculitis affecting the central nervous system. Cleve Clin J Med. 2002;69(suppl 2):SII105–SII108. - PubMed
-
- Volcy M, Toro ME, Uribe CS, Toro G. Primary angiitis of the central nervous system: report of five biopsy-confirmed cases from Colombia. J Neurol Sci. 2004;227:85–89. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
