

Subject-ventilator synchrony during neural versus pneumatically triggered non-invasive helmet ventilation
- PMID: 18512045
- PMCID: PMC2517084
- DOI: 10.1007/s00134-008-1163-z
Subject-ventilator synchrony during neural versus pneumatically triggered non-invasive helmet ventilation
Abstract
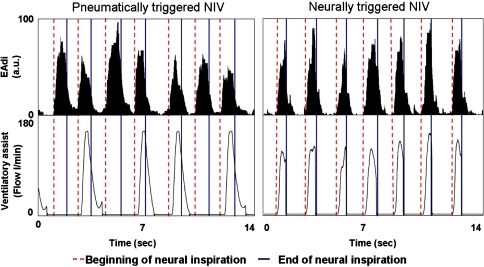
Objective: Patient-ventilator synchrony during non-invasive pressure support ventilation with the helmet device is often compromised when conventional pneumatic triggering and cycling-off were used. A possible solution to this shortcoming is to replace the pneumatic triggering with neural triggering and cycling-off-using the diaphragm electrical activity (EA(di)). This signal is insensitive to leaks and to the compliance of the ventilator circuit.
Design: Randomized, single-blinded, experimental study.
Setting: University Hospital. PARTICIPANTS AND SUBJECTS: Seven healthy human volunteers.
Interventions: Pneumatic triggering and cycling-off were compared to neural triggering and cycling-off during NIV delivered with the helmet.
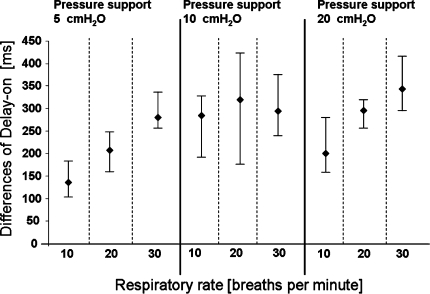
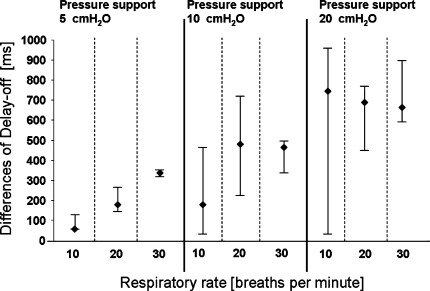
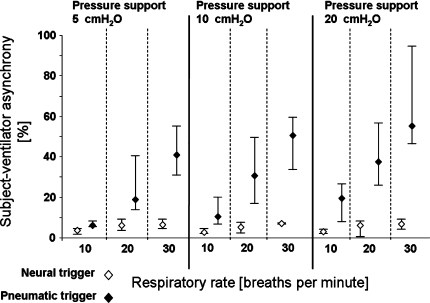
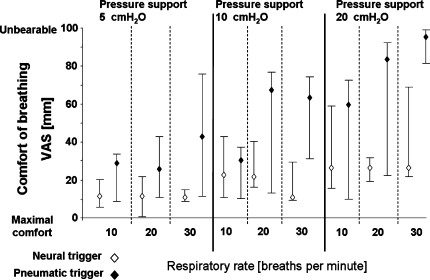
Measurements and results: Triggering and cycling-off delays, wasted efforts, and breathing comfort were determined during restricted breathing efforts (<20% of voluntary maximum EA(di)) with various combinations of pressure support (PSV) (5, 10, 20 cm H(2)O) and respiratory rates (10, 20, 30 breath/min). During pneumatic triggering and cycling-off, the subject-ventilator synchrony was progressively more impaired with increasing respiratory rate and levels of PSV (p < 0.001). During neural triggering and cycling-off, effect of increasing respiratory rate and levels of PSV on subject-ventilator synchrony was minimal. Breathing comfort was higher during neural triggering than during pneumatic triggering (p < 0.001).
Conclusions: The present study demonstrates in healthy subjects that subject-ventilator synchrony, trigger effort, and breathing comfort with a helmet interface are considerably less impaired during increasing levels of PSV and respiratory rates with neural triggering and cycling-off, compared to conventional pneumatic triggering and cycling-off.
Figures
Comment in
-
Neural trigger and cycling off during helmet pressure support ventilation: the epitome of the perfect patient ventilator interaction?Intensive Care Med. 2008 Sep;34(9):1562-4. doi: 10.1007/s00134-008-1164-y. Epub 2008 May 30. Intensive Care Med. 2008. PMID: 18512044 No abstract available.
References
-
- Carlucci A, Richard JC, Wysocki M, Lepage E, Brochard L. Noninvasive versus conventional mechanical ventilation. An epidemiologic survey. Am J Respir Crit Care Med. 2001;163:874–880. - PubMed
-
- Ram FS, Picot J, Lightowler J, Wedzicha JA. Non-invasive positive pressure ventilation for treatment of respiratory failure due to exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2004;3:CD004104. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
