

Abnormal body composition phenotypes in older rheumatoid arthritis patients: association with disease characteristics and pharmacotherapies
- PMID: 18512711
- PMCID: PMC2670994
- DOI: 10.1002/art.23719
Abnormal body composition phenotypes in older rheumatoid arthritis patients: association with disease characteristics and pharmacotherapies
Abstract
Objective: To compare measures of body fat and lean mass and the prevalence of abnormal body composition phenotypes (sarcopenia, overfat, and sarcopenic obesity) in men and women with rheumatoid arthritis (RA) versus matched controls, and to explore the disease-related predictors of abnormal body composition in patients with RA.
Methods: A total of 189 men and women with RA and 189 age-, sex-, and race-matched non-RA controls underwent dual-energy x-ray absorptiometry for measurement of total and regional body fat and lean mass. Continuous and categorical measures of body composition were compared between RA and control subjects by sex and according to categories of body mass index (BMI). Within the group of RA patients, demographic, lifestyle, and RA disease and treatment characteristics were compared for RA patients with healthy body composition versus those with abnormal body composition phenotypes.
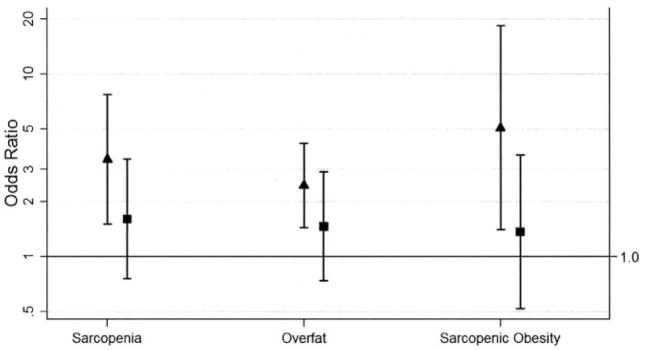
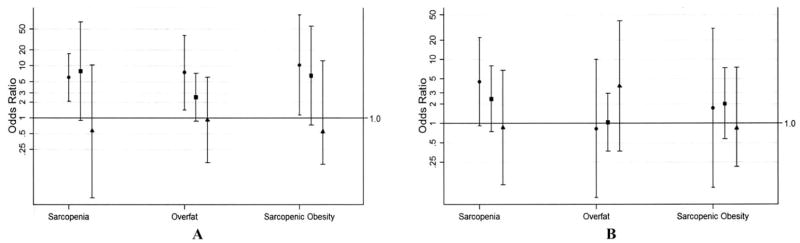
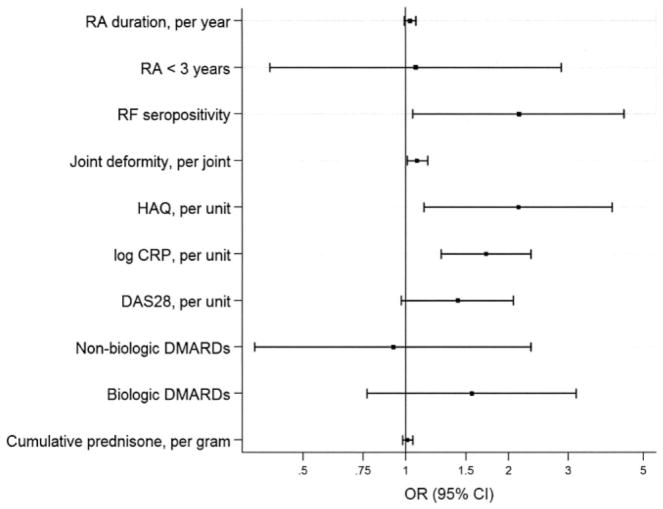
Results: Compared with non-RA controls, RA status was significantly associated with greater odds of sarcopenia, overfat, and sarcopenic obesity in women, but not in men. Relative differences in body composition phenotypes between RA and control subjects were greatest for patients in the normal weight BMI category (<25 kg/m(2)). Among RA characteristics, increasing joint deformity, self-reported disability scores, C-reactive protein levels, rheumatoid factor seropositivity, and a lack of current treatment with disease-modifying antirheumatic drugs were significantly associated with abnormal body composition.
Conclusion: Abnormal body composition phenotypes are overrepresented in patients with RA, particularly in those in the normal weight BMI range. RA-associated disease and treatment characteristics contribute to this increase in abnormal body composition.
Figures
References
-
- Paget J. Clinical lectures on the nervous mimicry of diseases: mimicry of diseases of joints. Lancet. 1873;102:727–9.
-
- Westhovens R, Nijs J, Taelman V, Dequeker J. Body composition in rheumatoid arthritis. Br J Rheumatol. 1997;36:444–8. - PubMed
-
- Janssen I. Influence of sarcopenia on the development of physical disability: the Cardiovascular Health Study. J Am Geriatr Soc. 2006;54:56–62. - PubMed
-
- Baumgartner RN, Wayne SJ, Waters DL, Janssen I, Gallagher D, Morley JE. Sarcopenic obesity predicts instrumental activities of daily living disability in the elderly. Obes Res. 2004;12:1995–2004. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
