

Race and the natural history of chronic heart failure: a propensity-matched study
- PMID: 18514928
- PMCID: PMC2771183
- DOI: 10.1016/j.cardfail.2008.02.004
Race and the natural history of chronic heart failure: a propensity-matched study
Abstract
Background: Racial differences in the epidemiology and outcomes of heart failure are well known. However, the association of race with the natural history of heart failure has not been previously studied in a propensity-matched population of chronic heart failure in which all measured baseline patient characteristics are well-balanced between the races.
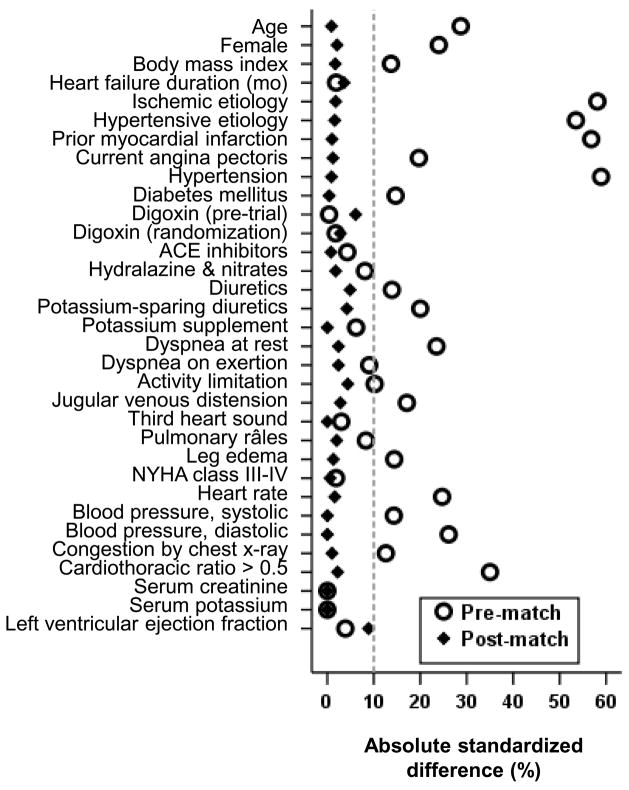
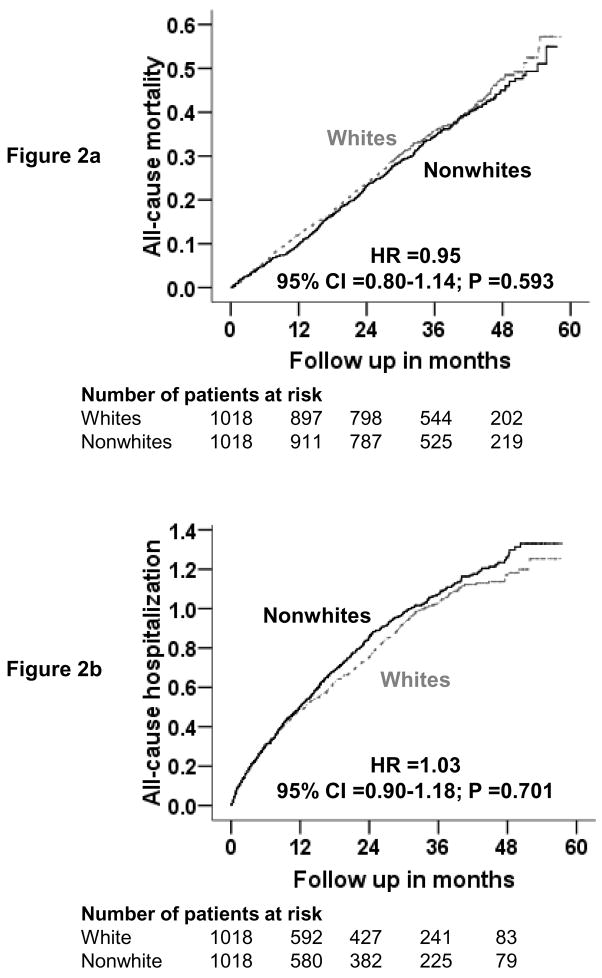
Methods and results: Of the 7788 patients with chronic systolic and diastolic heart failure in the Digitalis Investigation Group trial, 1128 were nonwhites. Propensity scores for being nonwhite were calculated for each patient and were used to match 1018 pairs of white and nonwhite patients. Matched Cox regression analyses were used to estimate associations of race with outcomes during 38 months of median follow-up. All-cause mortality occurred in 34% (rate, 1180/10000 person-years) of whites and 33% (rate, 1130/10000 person-years) of nonwhite patients (hazard ratio when nonwhite patients were compared with whites, 0.95, 95% confidence interval, 0.80-1.14; P = .593). All-cause hospitalization occurred in 63% (rate, 3616/10000 person-years) of whites and 65% (rate, 3877/10000 person-years) of nonwhite patients (hazard ratio, 1.03, 95% confidence interval, 0.90-1.18; P = .701). Respective hazard ratios (95% confidence intervals) for other outcomes were: 0.95 (0.75-1.12) for cardiovascular mortality, 0.82 (0.60-1.11) for heart failure mortality, 1.05 (0.91-1.22) for cardiovascular hospitalization, and 1.17 (0.98-1.39) for heart failure hospitalization.
Conclusions: In a propensity-matched population of heart failure patients where whites and nonwhites were balanced in all measured baseline characteristics, there were no racial differences in major natural history end points.
Conflict of interest statement
Figures
References
-
- Yancy CW. Heart failure in blacks: etiologic and epidemiologic differences. Curr Cardiol Rep. 2001;3:191–197. - PubMed
-
- Yancy CW. The role of race in heart failure therapy. Curr Cardiol Rep. 2002;4:218–225. - PubMed
-
- Yancy CW. Heart failure in African Americans. Am J Cardiol. 2005;96:3i–12i. - PubMed
-
- Deswal A, Petersen NJ, Urbauer DL, Wright SM, Beyth R. Racial variations in quality of care and outcomes in an ambulatory heart failure cohort. Am Heart J. 2006;152:348–354. - PubMed
-
- East MA, Peterson ED, Shaw LK, Gattis WA, O’Connor CM. Racial differences in the outcomes of patients with diastolic heart failure. Am Heart J. 2004;148:151–156. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
