

Anticipation of distress after discontinuation of mechanical ventilation in the ICU at the end of life
- PMID: 18516588
- PMCID: PMC2517089
- DOI: 10.1007/s00134-008-1172-y
Anticipation of distress after discontinuation of mechanical ventilation in the ICU at the end of life
Abstract
Background: A considerable number of patients admitted to the intensive care unit (ICU) die following withdrawal of mechanical ventilation. After discontinuation of ventilation without proper preparation, excessive respiratory secretion is common, resulting in a 'death rattle'. Post-extubation stridor can give rise to the relatives' perception that the patient is choking and suffering. Existing protocols lack adequate anticipatory preparation to respond to all distressing symptoms.
Methods: We analyzed existing treatment strategies in distressing symptoms after discontinuation of mechanical ventilation.
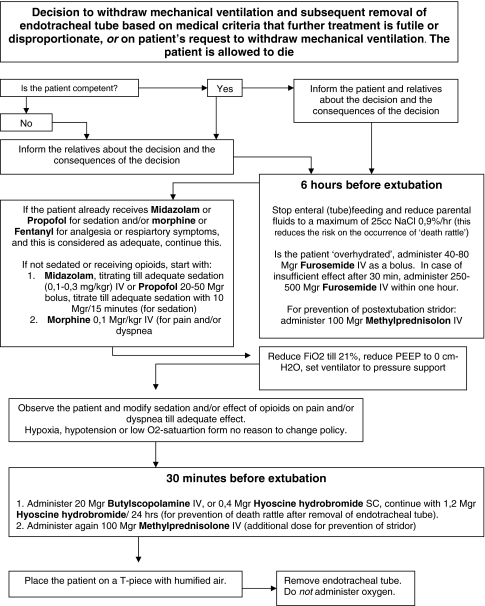
Conclusion: The actual period of discontinuation of mechanical ventilation can be very short, but thoughtful anticipation of distressing symptoms takes time. There is an ethical responsibility to anticipate and treat (iatrogenic) symptoms such as pain, dyspnea-associated respiratory distress, anxiety, delirium, post-extubation stridor, and excessive broncho-pulmonary secretions. This makes withdrawal of mechanical ventilation in ICU patients a thoughtful process, taking palliative actions instead of fast terminal actions. We developed a flowchart covering all possible distressing symptoms that can occur after withdrawal of mechanical ventilation and extubation. We recommend a two-phase process. Six hours before extubation, enteral feeding should be stopped and parenteral fluids reduced, overhydrated patients should be dehydrated with furosemide, administration of sedatives (for distress) and opioids (for pain and/or dyspnea) should be continued or started and methylprednisolone should be given in anticipation of stridor after extubation. Thirty minutes before extubation, Butylscopolamine should be given and methylprednisolone repeated. After this the patient should be extubated to secure a dying process as natural as possible with the lowest burden due to distress.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
