

Bone metabolism in adolescent athletes with amenorrhea, athletes with eumenorrhea, and control subjects
- PMID: 18519482
- PMCID: PMC3208310
- DOI: 10.1542/peds.2007-2392
Bone metabolism in adolescent athletes with amenorrhea, athletes with eumenorrhea, and control subjects
Abstract
Objective: We hypothesized that, despite increased activity, bone density would be low in athletes with amenorrhea, compared with athletes with eumenorrhea and control subjects, because of associated hypogonadism and would be associated with a decrease in bone formation and increases in bone-resorption markers.
Methods: In a cross-sectional study, we examined bone-density measures (spine, hip, and whole body) and body composition by using dual-energy radiograph absorptiometry and assessed fasting levels of insulin-like growth factor I and bone-turnover markers (N-terminal propeptied of type 1 procollagen and N-telopeptide) in 21 athletes with amenorrhea, 18 athletes with eumenorrhea, and 18 control subjects. Subjects were 12 to 18 years of age and of comparable chronologic and bone age.
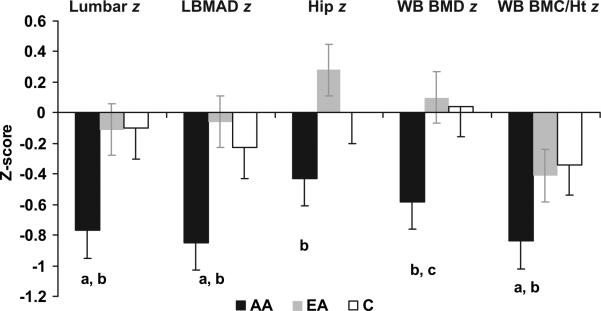
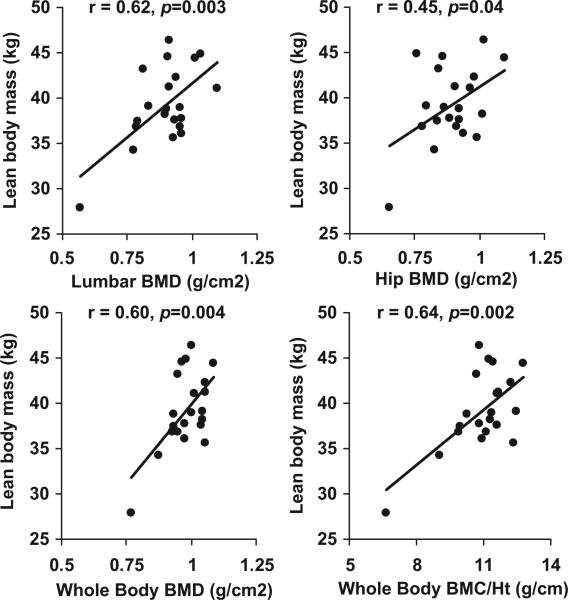
Results: Athletes with amenorrhea had lower bone-density z scores at the spine and whole body, compared with athletes with eumenorrhea and control subjects, and lower hip z scores, compared with athletes with eumenorrhea. Lean mass did not differ between groups. However, athletes with amenorrhea had lower BMI z scores than did athletes with eumenorrhea and lower insulin-like growth factor I levels than did control subjects. Levels of both markers of bone turnover were lower in athletes with amenorrhea than in control subjects. BMI z scores, lean mass, insulin-like growth factor I levels, and diagnostic category were important independent predictors of bone mineral density z scores.
Conclusions: Although they showed no significant differences in lean mass, compared with athletes with eumenorrhea and control subjects, athletes with amenorrhea had lower bone density at the spine and whole body. Insulin-like growth factor I levels, body-composition parameters, and menstrual status were important predictors of bone density. Follow-up studies are necessary to determine whether amenorrhea in athletes adversely affects the rate of bone mass accrual and therefore peak bone mass.
Figures
References
-
- Nichols JF, Rauh MJ, Lawson MJ, Ji M, Barkai HS. Prevalence of the female athlete triad syndrome among high school athletes. Arch Pediatr Adolesc Med. 2006;160(2):137–142. - PubMed
-
- Loucks A, Horvath S. Athletic amenorrhea: a review. Med Sci Sports Exerc. 1985;17(1):56–72. - PubMed
-
- Otis C. Exercise-associated amenorrhea. Clin Sports Med. 1992;11(2):351–362. - PubMed
-
- Shangold M, Rebar R, Wentz A, Schiff I. Evaluation and management of menstrual dysfunction in athletes. JAMA. 1990;263(12):1665–1669. - PubMed
-
- Loud KJ, Gordon CM, Micheli LJ, Field AE. Correlates of stress fractures among preadolescent and adolescent girls. Pediatrics. 2005;(4):115. Available at: www.pediatrics.org/cgi/content/full/115/4/e399. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
