

Postdischarge thromboprophylaxis and mortality risk after hip-or knee-replacement surgery
- PMID: 18519902
- PMCID: PMC2396368
- DOI: 10.1503/cmaj.071388
Postdischarge thromboprophylaxis and mortality risk after hip-or knee-replacement surgery
Erratum in
- CMAJ. 2008 Jul 1;179(1):56
Abstract
Background: Patients undergoing hip or knee replacement are at high risk of developing a postoperative venous thromboembolism even after discharge from hospital. We sought to identify hospital and patient characteristics associated with receiving thromboprophylaxis after discharge and to compare the risk of short-term mortality among those who did or did not receive thromboprophylaxis.
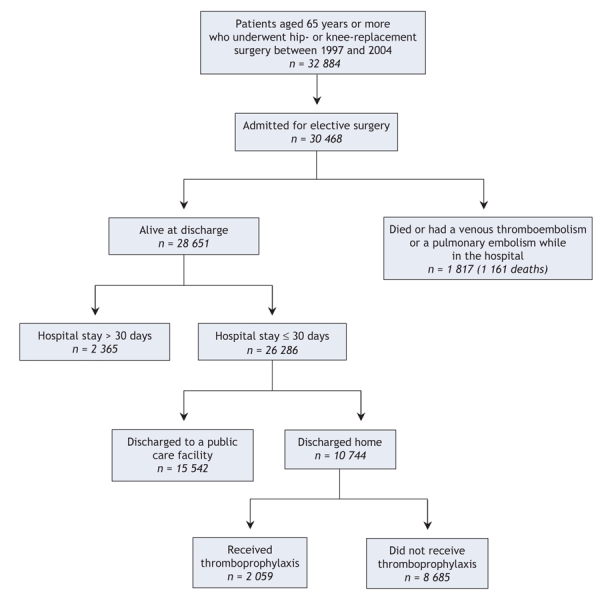
Methods: We conducted a retrospective cohort study using system-wide hospital discharge summary records, physician billing information, medication reimbursement claims and demographic records. We included patients aged 65 years and older who received a hip or knee replacement and who were discharged home after surgery.
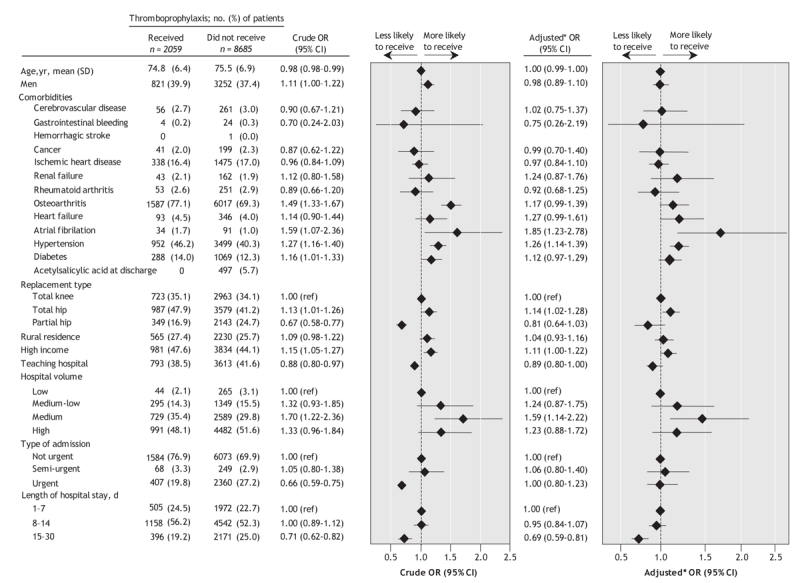
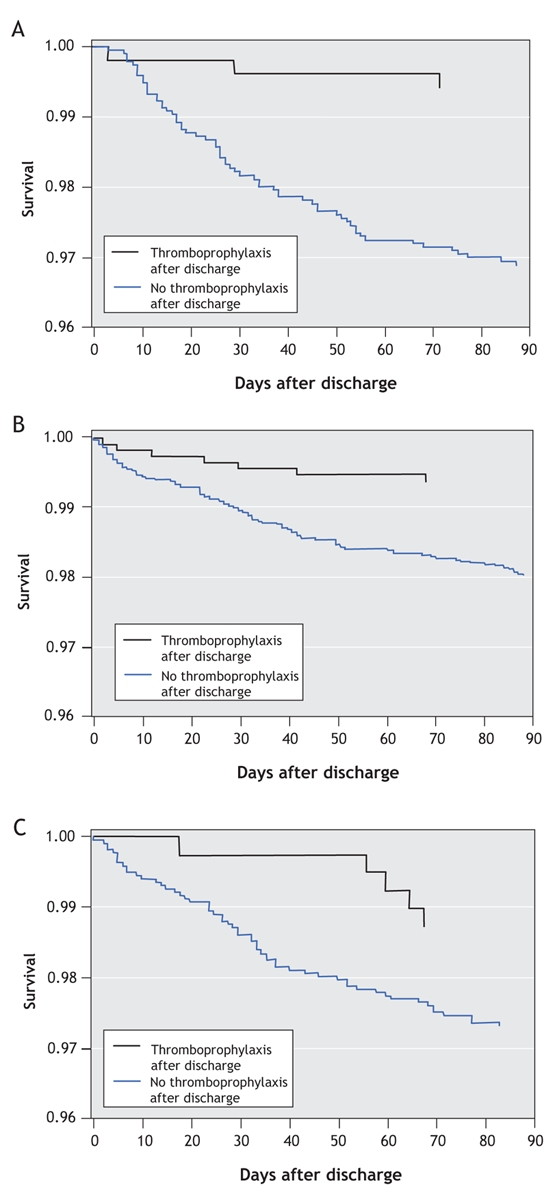
Results: In total we included 10 744 patients. Of these, 7058 patients who received a hip replacement and 3686 who received a knee replacement. The mean age was 75.4 (standard deviation [SD] 6.8) years and 38% of patients were men. In total, 2059 (19%) patients received thomboprophylaxis at discharge. Patients discharged from university teaching hospitals were less likely than those discharged from community hospitals to received thromboprophylaxis after discharge (odds ratio [OR] 0.89, 95% confidence interval [CI] 0.80-1.00). Patients were less likely to receive thromboprophylaxis after discharge if they had a longer hospital stay (15-30 days v. 1-7 days, OR 0.69, 95% CI 0.59-0.81). Patients were more likely to receive thromboprophylaxis if they had hip (v. knee) replacement, osteoarthritis, heart failure, atrial fibrillation or hypertension, higher (v. lower) income or if they were treated at medium-volume hospitals (69-116 hip and knee replacements per year). In total, 223 patients (2%) died in the 3-month period after discharge. The risk of short-term mortality was lower among those who received thromboprophylaxis after discharge (hazard ratio [HR] 0.34, 95% CI 0.20-0.57).
Interpretation: Fewer than 1 in 5 elderly patients discharged home after a hip-or knee-replacement surgery received postdischarge thromboprophylaxis. Those prescribed these medications had a lower risk of short-term mortality. The benefits of and barriers to thromboprophylaxis therapy after discharge in this population requires further study.
Figures
Comment in
-
Outpatient thromboprophylaxis after hip or knee surgery: discrepancies and concerns.CMAJ. 2008 Jun 3;178(12):1571-2. doi: 10.1503/cmaj.080507. CMAJ. 2008. PMID: 18519905 Free PMC article. Review. No abstract available.
Similar articles
-
Aspirin Compared with Anticoagulation to Prevent Venous Thromboembolism After Knee or Hip Arthroplasty: a Large Retrospective Cohort Study.J Gen Intern Med. 2019 Oct;34(10):2038-2046. doi: 10.1007/s11606-019-05122-3. Epub 2019 Jun 24. J Gen Intern Med. 2019. PMID: 31236894 Free PMC article.
-
Thromboprophylaxis following hip and knee arthroplasty.Intern Med J. 2013 Feb;43(2):124-9. doi: 10.1111/j.1445-5994.2013.02864.x. Intern Med J. 2013. PMID: 23402484
-
Venous Thromboembolism in Total Hip and Total Knee Arthroplasty.JAMA Netw Open. 2023 Dec 1;6(12):e2345883. doi: 10.1001/jamanetworkopen.2023.45883. JAMA Netw Open. 2023. PMID: 38039005 Free PMC article.
-
Factors associated with hospital stay length, discharge destination, and 30-day readmission rate after primary hip or knee arthroplasty: Retrospective Cohort Study.Orthop Traumatol Surg Res. 2019 Sep;105(5):949-955. doi: 10.1016/j.otsr.2019.04.012. Epub 2019 Jun 15. Orthop Traumatol Surg Res. 2019. PMID: 31208932 Review.
-
Clinical Effectiveness and Safety of Aspirin for Venous Thromboembolism Prophylaxis After Total Hip and Knee Replacement: A Systematic Review and Meta-analysis of Randomized Clinical Trials.JAMA Intern Med. 2020 Mar 1;180(3):376-384. doi: 10.1001/jamainternmed.2019.6108. JAMA Intern Med. 2020. PMID: 32011647 Free PMC article.
Cited by
-
Simplifying thromboprophylaxis could improve outcomes in orthopaedic surgery.Thrombosis. 2010;2010:108049. doi: 10.1155/2010/108049. Epub 2010 Sep 13. Thrombosis. 2010. PMID: 22084657 Free PMC article.
-
Rivaroxaban vs dabigatran for thromboprophylaxis after joint-replacement surgery: exploratory indirect comparison based on meta-analysis of pivotal clinical trials.Croat Med J. 2010 Apr;51(2):113-23. doi: 10.3325/cmj.2010.51.113. Croat Med J. 2010. PMID: 20401953 Free PMC article. Review.
-
Ten-Year Trends in Medical Complications Following 540,623 Primary Total Hip Replacements from a National Database.J Bone Joint Surg Am. 2018 Mar 7;100(5):360-367. doi: 10.2106/JBJS.16.01198. J Bone Joint Surg Am. 2018. PMID: 29509612 Free PMC article.
-
Outpatient thromboprophylaxis after hip or knee surgery: discrepancies and concerns.CMAJ. 2008 Jun 3;178(12):1571-2. doi: 10.1503/cmaj.080507. CMAJ. 2008. PMID: 18519905 Free PMC article. Review. No abstract available.
-
Pharmacological thromboprophylaxis and its impact on venous thromboembolism following total knee and hip arthroplasty in Korea: A nationwide population-based study.PLoS One. 2017 May 24;12(5):e0178214. doi: 10.1371/journal.pone.0178214. eCollection 2017. PLoS One. 2017. PMID: 28542415 Free PMC article.
References
-
- Geerts WH, Heit JA, Clagett GP, et al. Prevention of venous thromboembolism. Chest 2001;119:132S-75S. - PubMed
-
- Silverstein MD, Heit JA, Mohr DN, et al. Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med 1998;158:585-93. - PubMed
-
- Prevention of venous thromboembolism. International consensus statement (guidelines according to scientific evidence). Int Angiol 1997;16:3-38. - PubMed
-
- Pini M, Spyropoulos AC. Prevention of venous thromboembolism. Semin Thromb Hemost 2006;32:755-66. - PubMed
-
- Weinmann EE, Salzman EW. Deep-vein thrombosis. N Engl J Med 1994;331:1630-41. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical