

A cluster-randomized trial of provider-initiated (opt-out) HIV counseling and testing of tuberculosis patients in South Africa
- PMID: 18520677
- PMCID: PMC2632747
- DOI: 10.1097/QAI.0b013e3181775926
A cluster-randomized trial of provider-initiated (opt-out) HIV counseling and testing of tuberculosis patients in South Africa
Abstract
Objective: To determine whether implementation of provider-initiated human immunodeficiency virus (HIV) counseling would increase the proportion of tuberculosis (TB) patients who received HIV counseling and testing.
Design: Cluster-randomized trial with clinic as the unit of randomization.
Setting: Twenty, medium-sized primary care TB clinics in the Nelson Mandela Metropolitan Municipality, Port Elizabeth, Eastern Cape Province, South Africa.
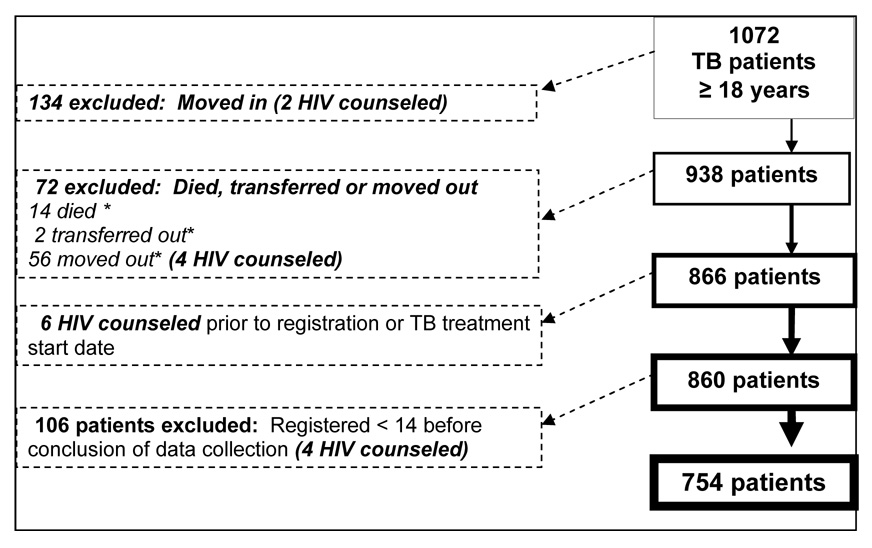
Subjects: A total of 754 adults (18 years and older) newly registered as TB patients in the 20 study clinics.
Intervention: Implementation of provider-initiated HIV counseling and testing.
Main outcome measures: Percentage of TB patients HIV counseled and tested. SECONDARY: Percentage of patients with HIV test positive, and percentage of those who received cotrimoxazole and who were referred for HIV care.
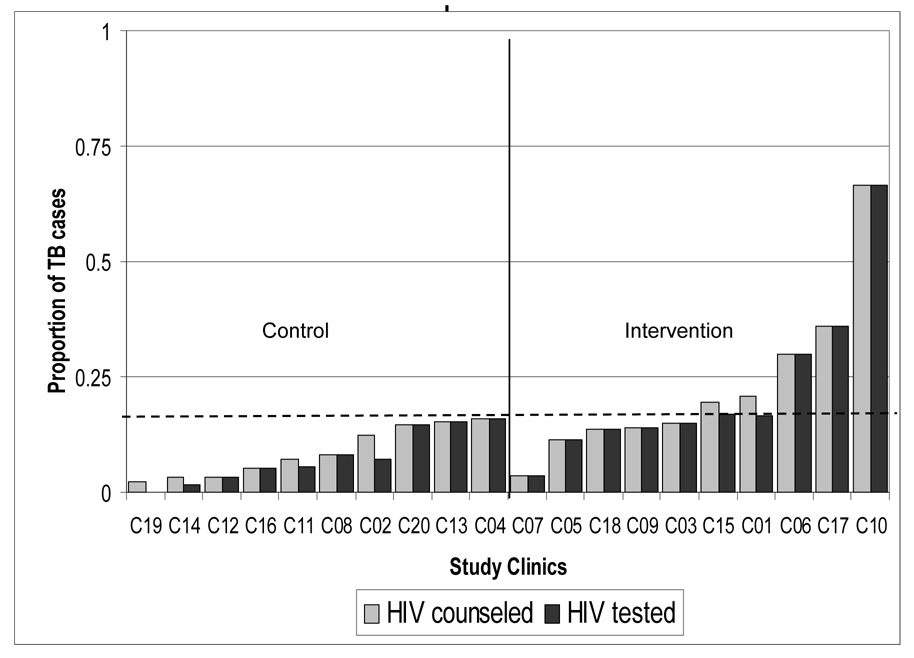
Results: : A total of 754 adults newly registered as TB patients were enrolled. In clinics randomly assigned to implement provider-initiated HIV counseling and testing, 20.7% (73/352) patients were counseled versus 7.7% (31/402) in the control clinics (P = 0.011), and 20.2% (n = 71) versus 6.5% (n = 26) underwent HIV testing (P = 0.009). Of those patients counseled, 97% in the intervention clinics accepted testing versus 79% in control clinics (P = 0.12). The proportion of patients identified as HIV infected in intervention clinics was 8.5% versus 2.5% in control clinics (P = 0.044). Fewer than 40% of patients with a positive HIV test were prescribed cotrimoxazole or referred for HIV care in either study arm.
Conclusions: Provider-initiated HIV counseling significantly increased the proportion of adult TB patients who received HIV counseling and testing, but the magnitude of the effect was small. Additional interventions to optimize HIV testing for TB patients urgently need to be evaluated.
Figures
References
-
- Chimzizi R, Gausi F, Bwanali A, et al. Voluntary counselling, HIV testing and adjunctive cotrimoxazole are associated with improved TB treatment outcomes under routine conditions in Thyolo District, Malawi. Int J Tuberc Lung Dis. 2004;8:579–585. - PubMed
-
- Chimzizi RB, Harries AD, Manda E, Khonyongwa A, Salaniponi FM. Counselling, HIV testing and adjunctive cotrimoxazole for TB patients in Malawi: from research to routine implementation. Int J Tuberc Lung Dis. 2004;8:938–944. - PubMed
-
- Desormeaux J, Johnson MP, Coberly JS, et al. Widespread HIV counseling and testing linked to a community-based tuberculosis control program in a high-risk population. Bull Pan Am Health Organ. 1996;30:1–8. - PubMed
-
- Hausler H. Lessons learned from ProTEST TB/HIV pilot districts in South Africa. ProTEST lessons learned workshop. Powerpoint presentation. 2003 February 3;
-
- Suggaravetsiri P, Yanai H, Chongsuvivatwong V, Naimpasan O, Akarasewi P. Integrated counseling and screening for tuberculosis and HIV among household contacts of tuberculosis patients in an endemic area of HIV infection: Chiang Rai, Thailand. Int J Tuberc Lung Dis. 2003;7:S424–S431. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
