

Selection of modalities, prescription, and technical issues in children on peritoneal dialysis
- PMID: 18521632
- PMCID: PMC2697927
- DOI: 10.1007/s00467-008-0848-4
Selection of modalities, prescription, and technical issues in children on peritoneal dialysis
Abstract
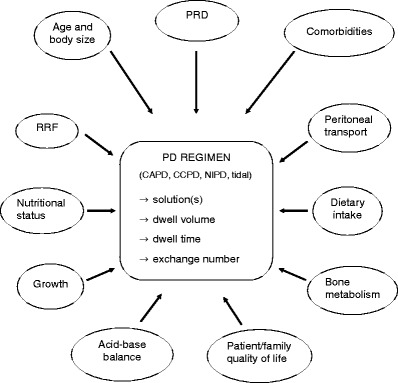
Peritoneal dialysis (PD) is widely employed as a dialytic therapy for uraemic children, especially in its automated form (APD), that is associated with less burden of care on patient and family than continuous ambulatory PD. Since APD offers a wide range of treatment options, based on intermittent and continuous regimens, prescription can be individualized according to patient's age, body size, residual renal function, nutritional intake, and growth-related metabolic needs. Transport capacity of the peritoneal membrane of each individual patient should be assessed, and regularly monitored, by means of standardized peritoneal function tests validated in pediatric patients. To ensure maximum recruitment of peritoneal exchange area, fill volume should be scaled to body surface area and adapted to each patient, according to clinical tolerance and intraperitoneal pressure. PD solutions should be employed according to their biocompatibility and potential ultrafiltration capacity; new pH-neutral, glucose-free solutions can be used in an integrated way in separate dwells, or by appropriately mixing during the same dialytic session. Kinetic modelling software programs may help in the tailoring of PD prescription to individual patients' characteristics and needs. Owing to advances in the technology of new APD machines, greater programming flexibility, memorized delivery control, and tele-dialysis are currently possible.
Figures
References
-
- Hattori S, Yosioka K, Honda M, Ito H. The 1998 report of the Japanese National Registry data on pediatric end-stage renal disease patients. Pediatr Nephrol. 2002;17:456–461. - PubMed
-
- Verrina E, Edefonti A, Gianoglio B, Rinaldi S, Sorino P, Zacchello G, Lavoratti G, Maringhini S, Pecoraro C, Calevo MG, Turrini Dertenois L, Perfumo F. A multicenter experience on patient and technique survival in children on chronic dialysis. Pediatr Nephrol. 2004;19:82–90. - PubMed
-
- Fadrowki JJ, Frankenfield D, Amaral S, Brady T, Gorman GH, Warady B, Furth SL, Fivush B, Neu AM. Children on long-term dialysis in the United States: findings from the 2005 ESRD Clinical Performance Measures Project. Am J Kidney Dis. 2007;50:958–966. - PubMed
-
- Fischbach M, Stefanidis CJ, Watson AR. Guidelines by an ad hoc European committee on adequacy of the pediatric peritoneal dialysis prescription. Nephrol Dial Transplant. 2002;17:380–385. - PubMed
-
- Morgestern B. Peritoneal dialysis and prescription monitoring. In: Warady BA, Schaefer FS, Fine RN, Alexander SR, editors. Pediatric dialysis. Dordrecht: Kluwer Academic Publishers; 2004. pp. 147–161.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
