

Characterization of virus-specific T-cell immunity in liver allograft recipients with HCV-induced cirrhosis
- PMID: 18522547
- PMCID: PMC2796869
- DOI: 10.1111/j.1600-6143.2008.02248.x
Characterization of virus-specific T-cell immunity in liver allograft recipients with HCV-induced cirrhosis
Abstract
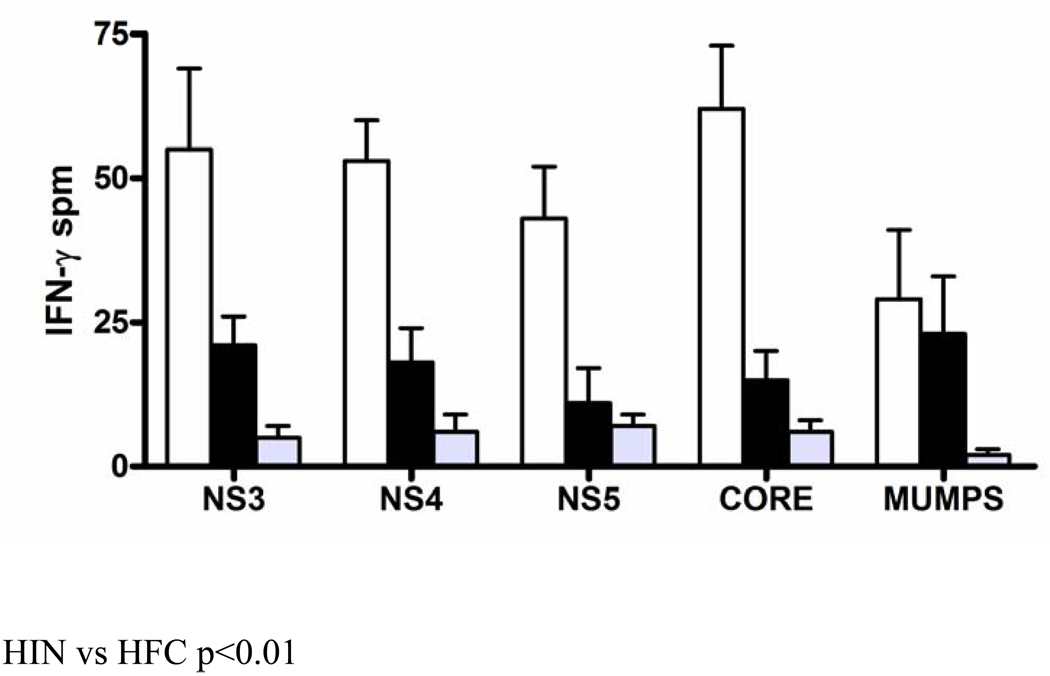
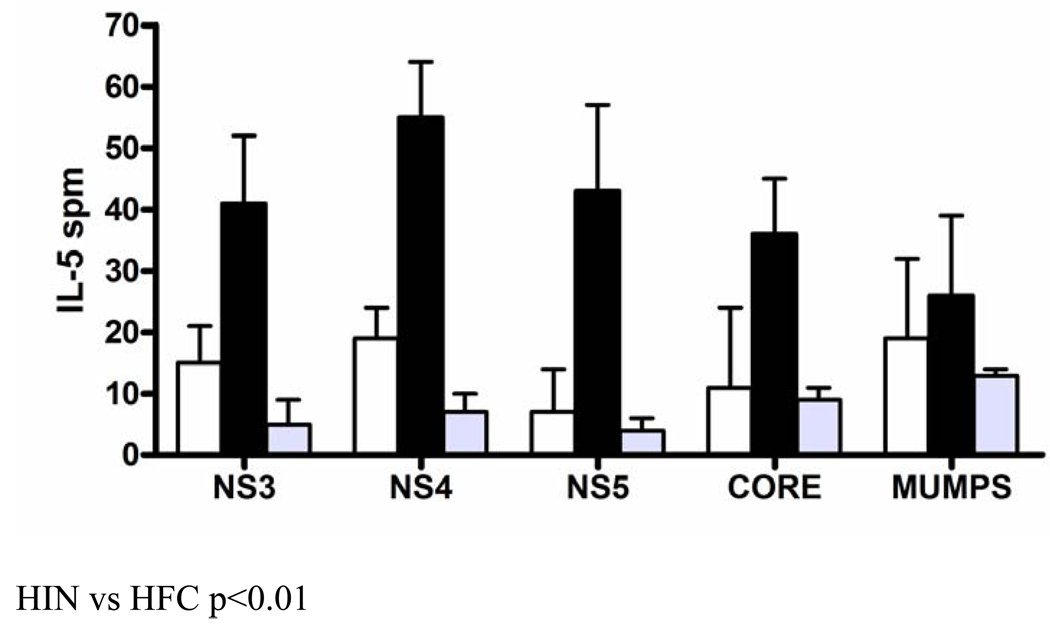
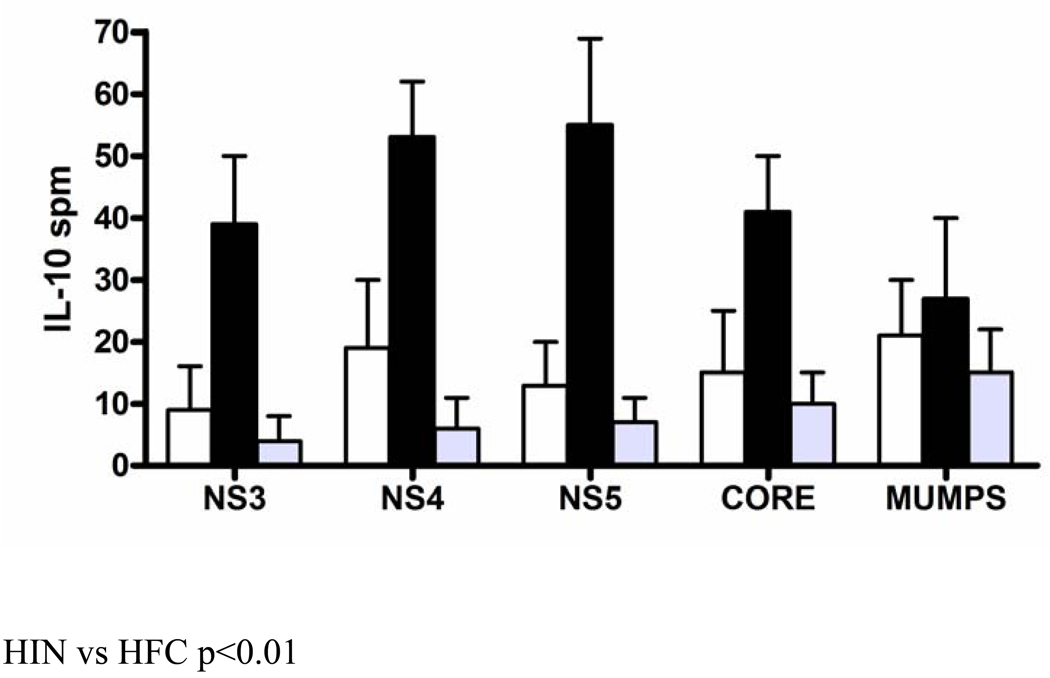
Recurrent hepatitis C infection (HCV) following liver transplantation causes accelerated allograft cirrhosis. Here we characterized HCV-specific immunity in adult liver transplant recipients (n = 74) with and without allograft cirrhosis. Patients were divided into hepatic inflammation/no cirrhosis (METAVIR scores 0-2, HIN) and hepatic cirrhosis (score 3-4, HFC). As control, 20 normal subjects and 10 non-HCV liver transplant patients were included. Twenty-five different serum cytokines were analyzed using LUMINEX. Frequency of T-cells specific to HCV-derived proteins (NS3, NS4, NS5, Core) was characterized using ELISPOT immunoassays. There was no difference in clinical characteristics between HIN (n = 49) and HFC (n = 25) groups. HIN group had high serum IFN-gamma and IL-12 while HFC demonstrated elevated IL-4, IL-5 and IL-10 (p < 0.01). HCV (NS3, NS4, NS5, Core)-specific IFN-gamma-producing CD4+ T-cells were elevated in the HIN group whereas the HFC patients showed predominance of HCV-specific IL-5 and IL-10-producing CD4+ T-cells.
Conclusions: Lack of HCV-specific Th1-type T-cell immunity is observed in liver transplant recipients with advanced allograft cirrhosis.
Figures
References
-
- Wright TL, Donegan E, Hsu HH, Ferrell L, Lake JR, Kim M, et al. Recurrent and acquired hepatitis C viral infection in liver transplant recipients. Gastroenterology. 1992;103(1):317–322. - PubMed
-
- Feray C, Gigou M, Samuel D, Paradis V, Wilber J, David MF, et al. The course of hepatitis C virus infection after liver transplantation. Hepatology. 1994;20(5):1137–1143. - PubMed
-
- Gane EJ, Naoumov NV, Qian KP, Mondelli MU, Maertens G, Portmann BC, et al. A longitudinal analysis of hepatitis C virus replication following liver transplantation. Gastroenterology. 1996;110(1):167–177. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
