

Population causes and consequences of leading chronic diseases: a comparative analysis of prevailing explanations
- PMID: 18522614
- PMCID: PMC2690359
- DOI: 10.1111/j.1468-0009.2008.00522.x
Population causes and consequences of leading chronic diseases: a comparative analysis of prevailing explanations
Abstract
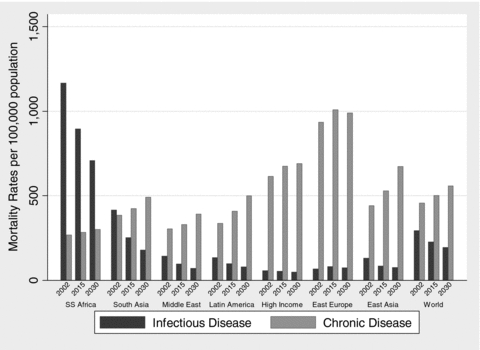
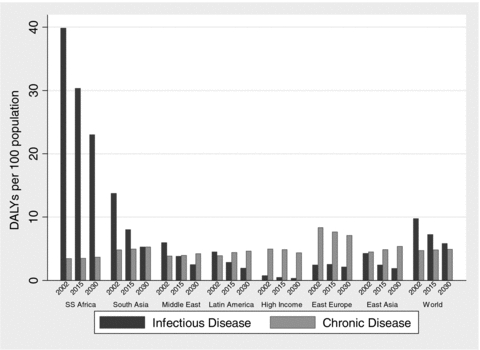
Context: The mortality numbers and rates of chronic disease are rising faster in developing than in developed countries. This article compares prevailing explanations of population chronic disease trends with theoretical and empirical models of population chronic disease epidemiology and assesses some economic consequences of the growth of chronic diseases in developing countries based on the experiences of developed countries.
Methods: Four decades of male mortality rates of cardiovascular and chronic noncommunicable diseases were regressed on changes in and levels of country income per capita, market integration, foreign direct investment, urbanization rates, and population aging in fifty-six countries for which comparative data were available. Neoclassical economic growth models were used to estimate the effect of the mortality rates of chronic noncommunicable diseases on economic growth in high-income OECD countries.
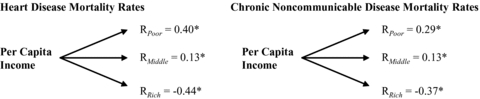
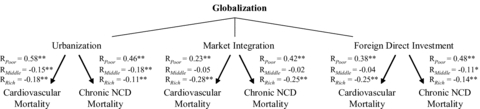
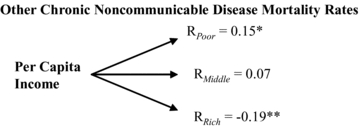
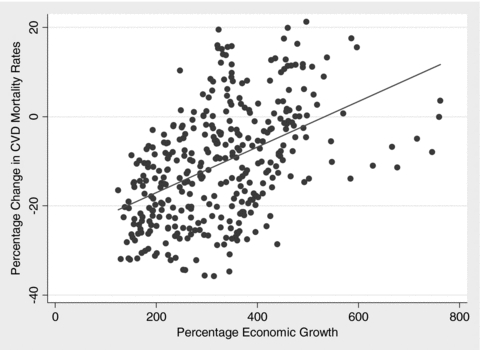
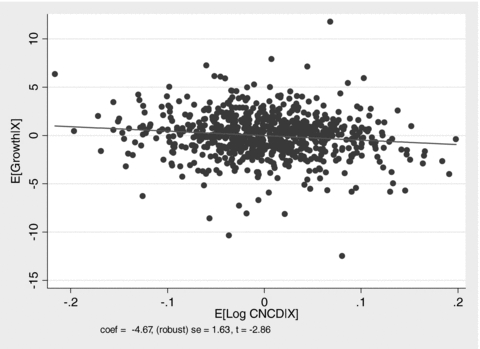
Findings: Processes of economic growth, market integration, foreign direct investment, and urbanization were significant determinants of long-term changes in mortality rates of heart disease and chronic noncommunicable disease, and the observed relationships with these social and economic factors were roughly three times stronger than the relationships with the population's aging. In low-income countries, higher levels of country income per capita, population urbanization, foreign direct investment, and market integration were associated with greater mortality rates of heart disease and chronic noncommunicable disease, less increased or sometimes reduced rates in middle-income countries, and decreased rates in high-income countries. Each 10 percent increase in the working-age mortality rates of chronic noncommunicable disease decreased economic growth rates by close to a half percent.
Conclusions: Macrosocial and macroeconomic forces are major determinants of population rises in chronic disease mortality, and some prevailing demographic explanations, such as population aging, are incomplete on methodological, empirical, and policy grounds. Rising chronic disease mortality rates will significantly reduce economic growth in developing countries and further widen the health and economic gap between the developed and developing world.
Figures
References
-
- Aboderin I, Kalache A, Ben-Shlomo Y, Lynch JW, Yajnik CS, Kuh D, Yach D. Life-Course Perspectives on Coronary Heart Disease, Stroke and Diabetes: Key Issues and Implications for Policy and Research. 2001. [accessed March 31, 2008]. Geneva: World Health Organization. Available at http://whqlibdoc.who.int/hq/2001/WHO_NMH_NPH_01.4.pdf.
-
- Bashar M, Alcabes P, Rom WN, Condos R. Increased Incidence of Multi-Drug Resistant Tuberculosis in Diabetic Patients on the Bellevue Chest Service, 1987 to 1997. Chest. 2001;120:1514–19. - PubMed
-
- Bates MN, Khalakdina A, Pai M, Change L, Lessa F, Smith KR. Risk of Tuberculosis from Exposure to Tobacco Smoke: A Systematic Review and Meta-Analysis. Archives of Internal Medicine. 2007;167(4):335. - PubMed
-
- Beaglehole R, Yach D. Globalisation and the Prevention and Control of Non-Communicable Disease: The Neglected Chronic Diseases of Adults. The Lancet. 2003;362(9387):903–8. - PubMed
-
- Beck N, Katz JN. What to Do (and Not to Do) with Time-Series Cross-Section Data. American Political Science Review. 1995;89:634–47.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
