

Combined written and oral information prior to gastrointestinal endoscopy compared with oral information alone: a randomized trial
- PMID: 18522729
- PMCID: PMC2430967
- DOI: 10.1186/1471-230X-8-22
Combined written and oral information prior to gastrointestinal endoscopy compared with oral information alone: a randomized trial
Abstract
Background: Little is known about how to most effectively deliver relevant information to patients scheduled for endoscopy.
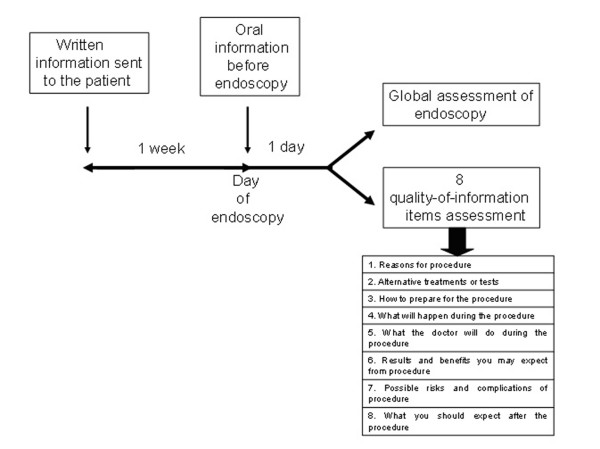
Methods: To assess the effects of combined written and oral information, compared with oral information alone on the quality of information before endoscopy and the level of anxiety. We designed a prospective study in two Swiss teaching hospitals which enrolled consecutive patients scheduled for endoscopy over a three-month period. Patients were randomized either to receiving, along with the appointment notice, an explanatory leaflet about the upcoming examination, or to oral information delivered by each patient's doctor. Evaluation of quality of information was rated on scales between 0 (none received) and 5 (excellent). The analysis of outcome variables was performed on the basis of intention to treat-analysis. Multivariate analysis of predictors of information scores was performed by linear regression analysis.
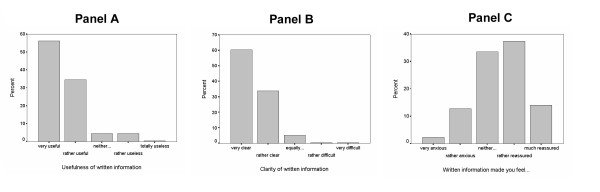
Results: Of 718 eligible patients 577 (80%) returned their questionnaire. Patients who received written leaflets (N = 278) rated the quality of information they received higher than those informed verbally (N = 299), for all 8 quality-of-information items. Differences were significant regarding information about the risks of the procedure (3.24 versus 2.26, p < 0.001), how to prepare for the procedure (3.56 versus 3.23, p = 0.036), what to expect after the procedure (2.99 versus 2.59, p < 0.001), and the 8 quality-of-information items (3.35 versus 3.02, p = 0.002). The two groups reported similar levels of anxiety before procedure (p = 0.66), pain during procedure (p = 0.20), tolerability throughout the procedure (p = 0.76), problems after the procedure (p = 0.22), and overall rating of the procedure between poor and excellent (p = 0.82).
Conclusion: Written information led to more favourable assessments of the quality of information and had no impact on patient anxiety nor on the overall assessment of the endoscopy. Because structured and comprehensive written information is perceived as beneficial by patients, gastroenterologists should clearly explain to their patients the risks, benefits and alternatives of endoscopic procedures.
Trial registration: Current Controlled trial number: ISRCTN34382782.
Figures
References
-
- Gerstenberger PD, Plumeri PA. Malpractice claims in gastrointestinal endoscopy; analysis of an insurance industry database. Gastrointest Endosc. 1993;39:132–8. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
