

Review
doi: 10.1016/j.cmet.2008.03.010.
Hypertension and cerebrovascular dysfunction
Affiliations
- PMID: 18522829
- PMCID: PMC2475602
- DOI: 10.1016/j.cmet.2008.03.010
Item in Clipboard
Review
Hypertension and cerebrovascular dysfunction
Cell Metab.
2008 Jun.
Abstract
Essential hypertension has devastating effects on the brain, being the major cause of stroke and a leading cause of dementia. Hypertension alters the structure of cerebral blood vessels and disrupts intricate vasoregulatory mechanisms that assure an adequate blood supply to the brain. These alterations threaten the cerebral blood supply and increase the susceptibility of the brain to ischemic injury as well as Alzheimer's disease. This review focuses on the mechanisms by which hypertension disrupts cerebral blood vessels, highlighting recent advances and outstanding issues.
Figures
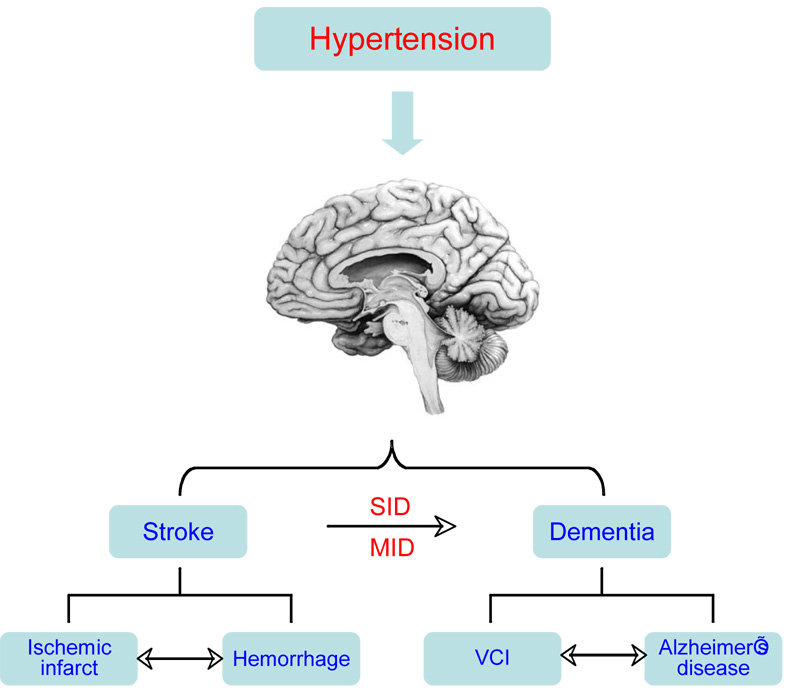
Hypertension has a key role in two major brain pathologies: stroke and dementia. Stroke can result from occlusion of a major cerebral artery (ischemic stroke) or rupture of intracerebral arterioles (hemorrhage). Hypertension also causes rupture of berry aneurysms of the circle of Willis leading to bleeding into the subarachnoid space (subarachnoid hemorrhage). Ischemia can lead to hemorrhage by rupture of ischemic vessels or extravasation of blood from leaky blood vessels. Conversely, hemorrhage can lead to ischemia by compressing the surrounding areas and reducing local blood flow. Vascular cognitive impairment (VCI) is caused by occlusion of small arterioles in the subcortical white matter, which interrupt neural connections subserving cognition and memory (Chui, 2007). A single stroke can lead to dementia by interrupting circuits involved in memory and cognition, such as the midline thalamus (strategic infarct dementia; SID). Multiple strokes can cause dementia by producing cumulative brain damage (multi infarct dementia; MID). Hypertension is a risk factor for Alzheimer’s disease (AD), a progressive dementia caused by accumulation of amyloid-β (Staessen et al., 2007). While vascular dementia and AD were traditionally considered separate entities, recent evidence suggests that they share common and interacting pathogenic factors (Iadecola, 2004).
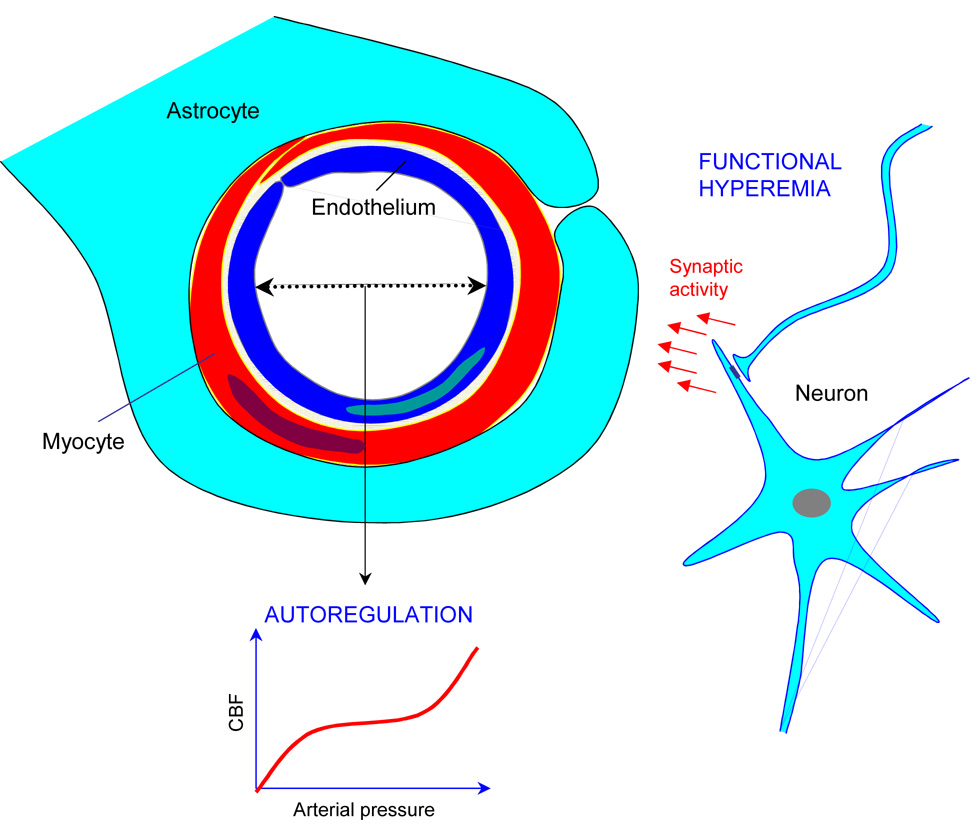
Neurons, astrocytes, myocytes and endothelial cells act in concert to maintain an adequate cerebral perfusion. Functional hyperemia increases CBF when neural activity increases. Cerebrovascular autoregulation maintains CBF stable during variations in arterial pressure within a certain range. Although not shown in this figure, larger cerebral arteries also contribute to autoregulation (see text). Endothelial cells release potent vasodilatator and constrictor agents in response to chemical and mechanical signals.
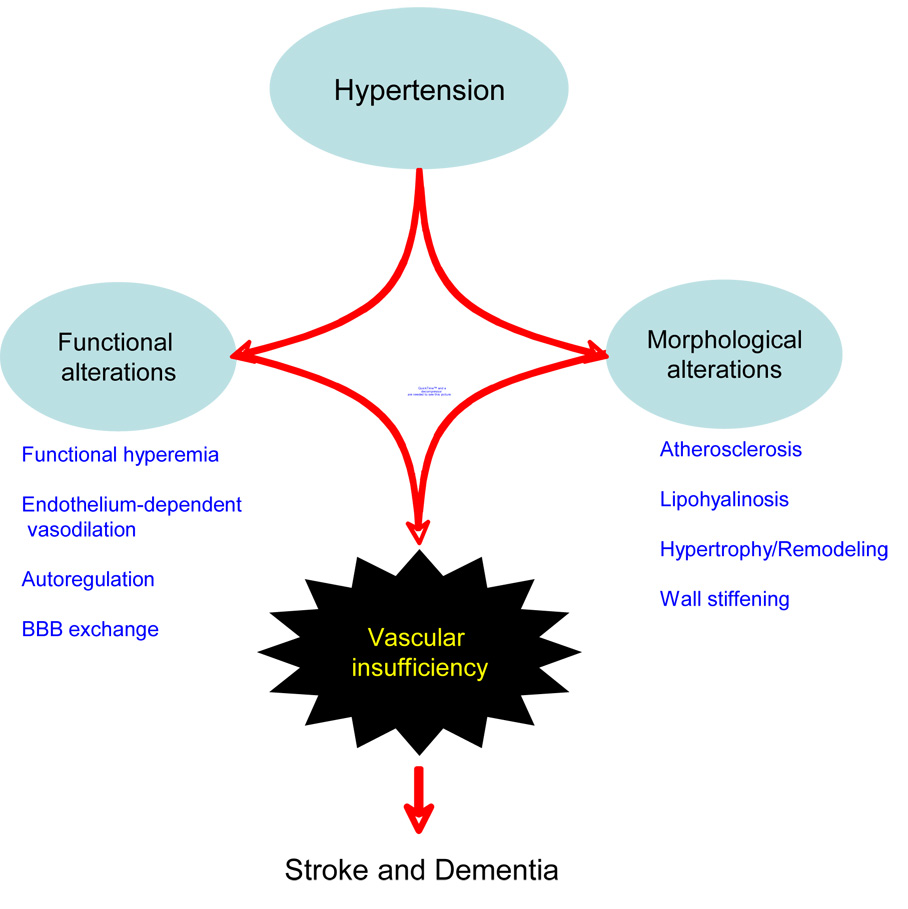
Hypertension induces structural and functional alterations in cerebral blood vessels, which compromise the blood supply to the brain and increase the risk of stroke and dementia. See text for details.
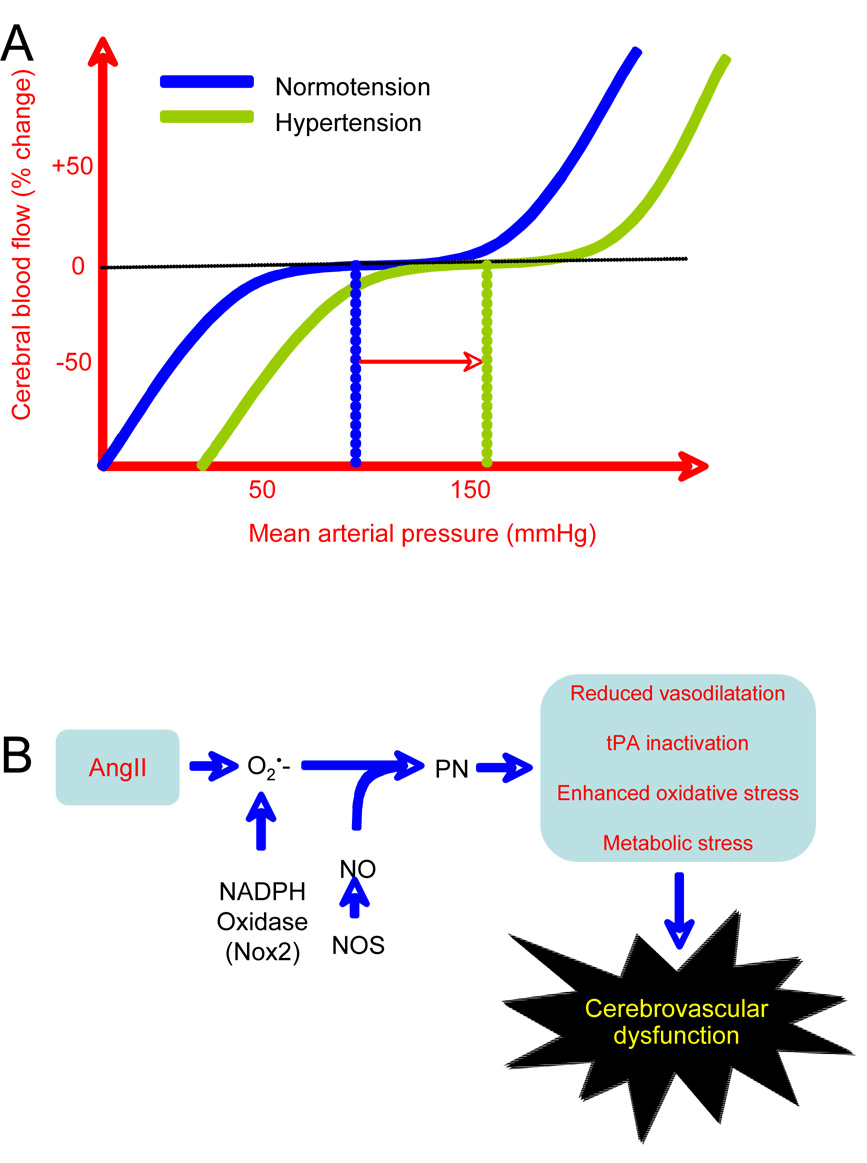
A. Cerebrovascular autoregulation: CBF is maintained relatively constant despite changes in arterial pressure within a certain range (60 to 150 mmHg mean arterial pressure). Hypertension shifts the curve to the right, so that higher levels of blood pressure are needed to maintain CBF in the autoregulated range. B. Peroxynitrite (PN) production mediates cerebrovascular dysfunction by AngII: PN formed from NADPH-derived superoxide and NO induces vascular dysfunction through different mechanisms (see (Pacher et al., 2007) for references): (1) PN opposes vasodilation by removing NO and by inhibiting prostacylin synthase, the enzyme that produces prostacyclin; (2) PN nitrates tPA and attenuates its proteolytic activity (Nielsen et al., 2004); (3) PN exacerbates oxidative stress by inhibiting SOD and by altering NOS to produce superoxide instead of NO (NOS uncoupling); (4) PN induces DNA damage leading to overactivation of the DNA repair enzyme poly(ADP)ribose polymerase resulting in NAD depletion and energy deficit; (5) PN inactivates mitochondrial enzymes and alcohol dehydrogenase, and can induce metabolic stress.
References
-
- Ago T, Kitazono T, Kuroda J, Kumai Y, Kamouchi M, Ooboshi H, Wakisaka M, Kawahara T, Rokutan K, Ibayashi S, et al. NAD(P)H oxidases in rat basilar arterial endothelial cells. Stroke. 2005;36:1040–1046. - PubMed
-
- Andresen J, Shafi NI, Bryan RM., Jr Endothelial influences on cerebrovascular tone. J Appl Physiol. 2006;100:318–327. - PubMed
-
- Barry DI. Cerebral blood flow in hypertension. J Cardiovasc Pharmacol. 1985;7 Suppl 2:S94–S98. - PubMed
-
- Baumbach GL, Didion SP, Faraci FM. Hypertrophy of cerebral arterioles in mice deficient in expression of the gene for CuZn superoxide dismutase. Stroke. 2006;37:1850–1855. - PubMed
-
- Baumbach GL, Heistad DD. Cerebral circulation in chronic arterial hypertension. Hypertension. 1988;12:89–95. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
