

Hypophosphatemic rickets with hypercalciuria due to mutation in SLC34A3/NaPi-IIc can be masked by vitamin D deficiency and can be associated with renal calcifications
- PMID: 18523928
- PMCID: PMC4777409
- DOI: 10.1055/s-2008-1076716
Hypophosphatemic rickets with hypercalciuria due to mutation in SLC34A3/NaPi-IIc can be masked by vitamin D deficiency and can be associated with renal calcifications
Abstract
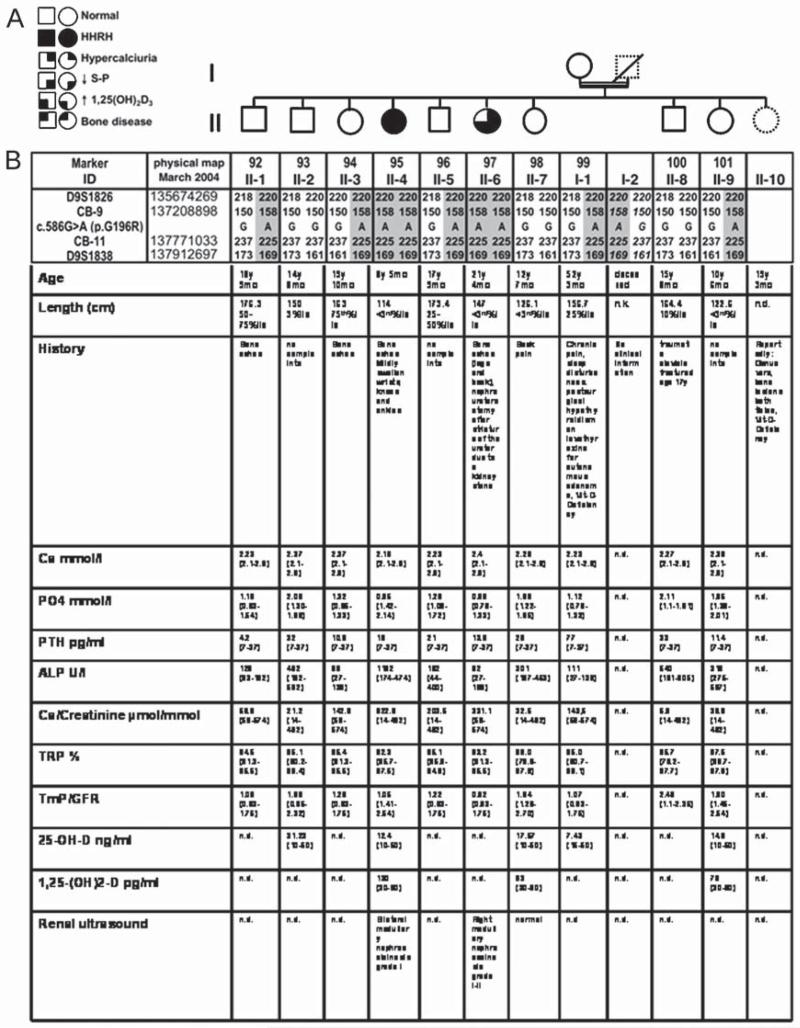
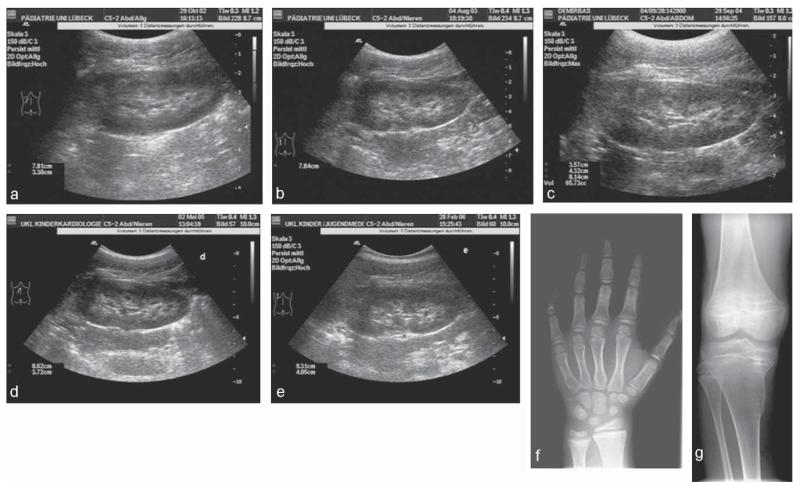
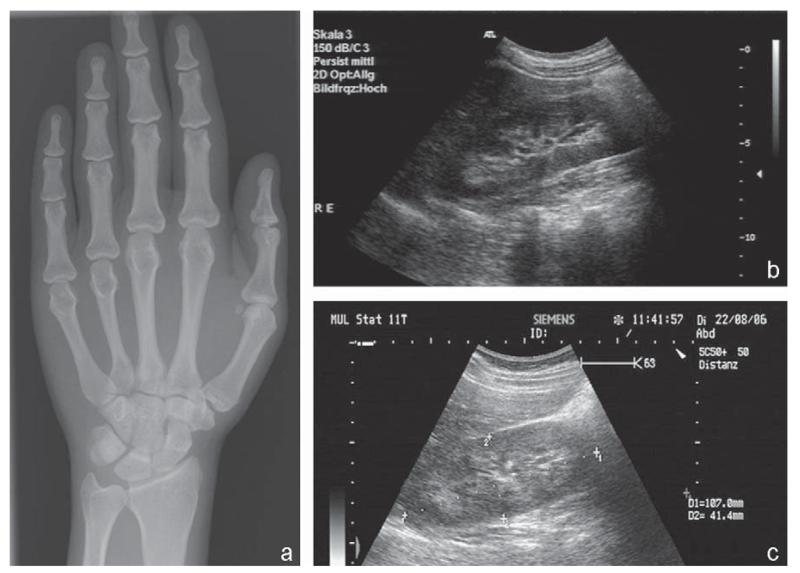
Hereditary hypophosphatemic rickets with hypercalciuria (HHRH) is caused by mutations in SLC34A3, the gene encoding the renal sodium-phosphate co-transporter NaPi-IIc. Despite increased urinary calcium excretion, HHRH is typically not associated with kidney stones prior to treatment. However, here we describe two sisters, who displayed nephrolithiasis or nephrocalcinosis upon presentation. The index patient, II-4, presented with short stature, bone pain, and knee X-rays suggestive of mild rickets at age 8.5 years. Laboratory evaluation showed hypophosphatemia, elevated 1,25(OH) (2) vitamin D levels, and hypercalciuria, later also developing vitamin D deficiency. Her sister, II-6, had a low normal serum phosphorous level, biochemically vitamin D deficiency and no evidence for osteomalacia, but had undergone left nephro-ureterectomy at age 17 because of ureteral stricture secondary to renal calculi. Nucleotide sequence analysis of DNA from II-4 and II-6 revealed a homozygous missense mutation c.586G>A (p.G196R) in SLC34A3/NaPi-IIc. Ultrasonographic examinations prior to treatment showed grade I nephrocalcinosis for II-4, while II-6 had grade I-II nephrocalcinosis in her remaining kidney. Four siblings and the mother were heterozygous carriers of the mutation, but showed no biochemical abnormalities. With oral phosphate supplements, hypophosphatemia and hypercalciuria improved in both homozygous individuals. Renal calcifications that are presumably due to increased urinary calcium excretion can be the presenting finding in homozygous carriers of G196R in SLC34A3/NaPi-IIc, and some or all laboratory features of HHRH may be masked by vitamin D deficiency.
Figures
References
-
- ADHR Consortium. White KE, Evans WE, O’Riordan JLH, Speer MC, Econs MJ, Lorenz-Depiereux B, Grabowski M, Mettinger T, Strom TM. Autosomal dominant hypophosphataemic rickets is associated with mutations in FGF23. Nat Genet. 2000;26:345–348. - PubMed
-
- Bacic D, Lehir M, Biber J, Kaissling B, Murer H, Wagner CA. The renal Na+/phosphate cotransporter NaPi-IIa is internalized via the receptor-mediated endocytic route in response to parathyroid hormone. Kidney Internl. 2006;69(3):495–503. - PubMed
-
- Ben-Ishay D, Dreyfuss F, Ullmann TD. Fanconi syndrome with hypouricemia in an adult: family study. Am J Med. 1961;31:793–800. - PubMed
-
- Bergwitz C, Roslin NM, Tieder M, Loredo-Osti JC, Bastepe M, Abu-Zahra H, Frappier D, Burkett K, Carpenter TO, Anderson D, Garabédian M, Sermet I, Fujiwara M, Morgan K, Tenenhouse HS, Jüppner H. SLC34A3 Mutations in patients with hereditary hypophosphataemic rickets with hypercalciuria predict a key role for the sodium-phosphate cotransporter NaPi-IIc in maintaining phosphate homeostasis. Am J Hum Genet. 2006;78(2):179–192. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
