

Neurosyphilis in a clinical cohort of HIV-1-infected patients
- PMID: 18525260
- PMCID: PMC2553365
- DOI: 10.1097/QAD.0b013e32830184df
Neurosyphilis in a clinical cohort of HIV-1-infected patients
Abstract
Objectives: To describe the risk factors, clinical presentation, and long-term follow up of patients enrolled in a clinical cohort of HIV-infected patients who were diagnosed and treated for neurosyphilis.
Methods: Comprehensive demographic, clinical, and therapeutic data were collected prospectively on all patients between 1990 and 2006. Patients were diagnosed with neurosyphilis if they had positive syphilis serologies and any of the following: (a) one or more cerebrospinal fluid abnormalities on lumbar puncture [white blood cells >10/microl; protein >50 mg/dl; reactive venereal diseases research laboratory], (b) an otherwise unexplained neurological finding.
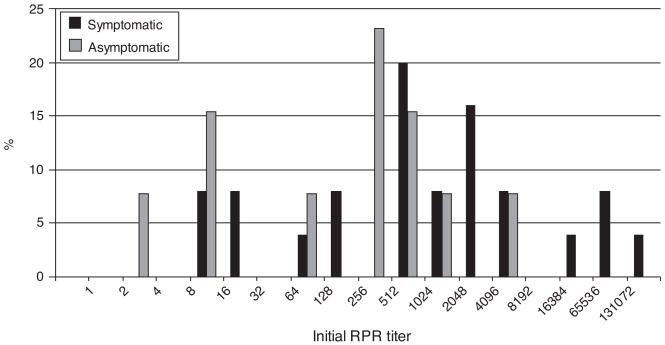
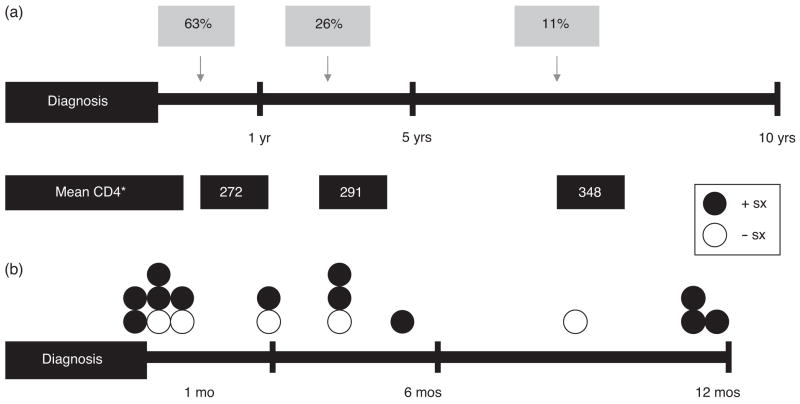
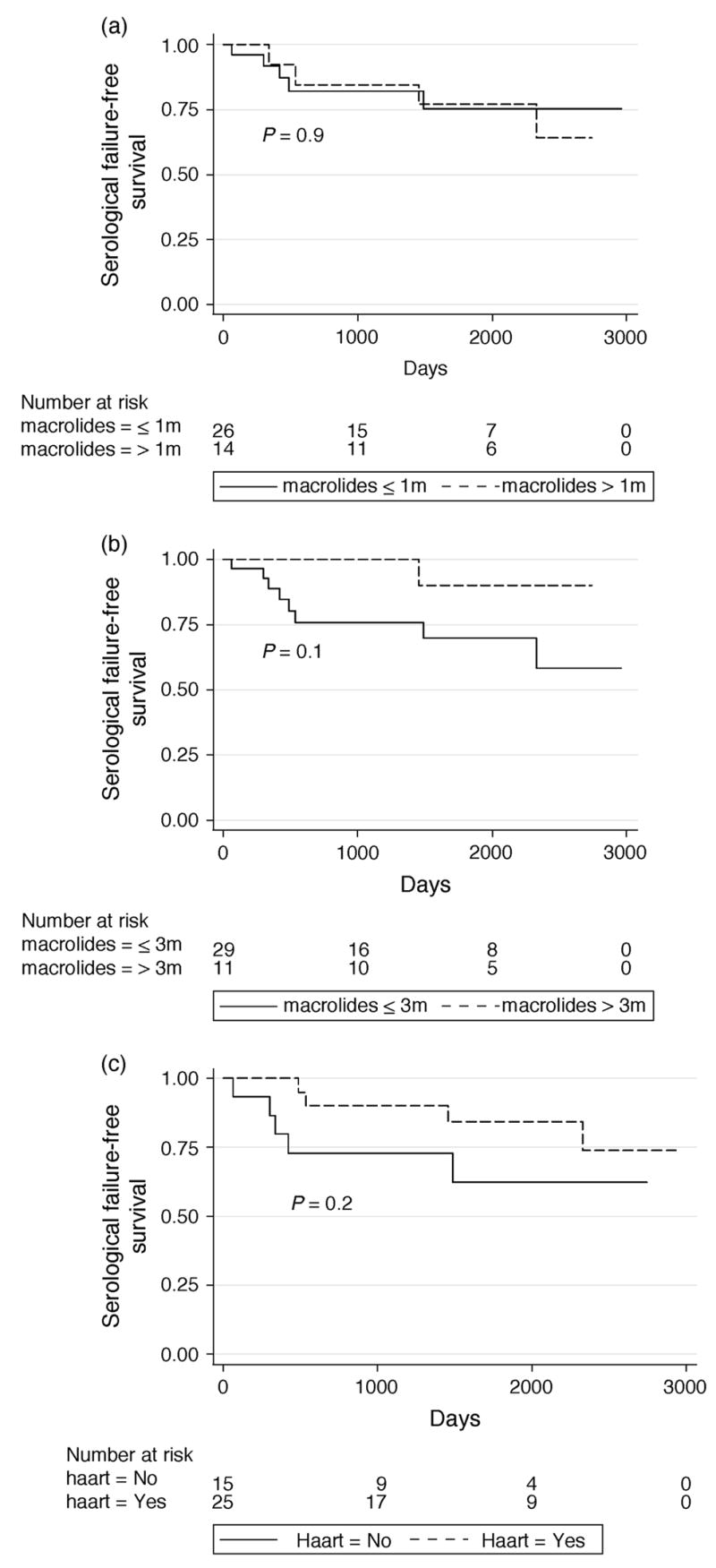
Results: Of 231 newly diagnosed syphilis cases, 41 neurosyphilis cases met entry criteria (median age 38.6 years, 79.1% male). Risk factors for neurosyphilis included a CD4 cell count of less than 350 cells/ml at the time of syphilis diagnosis (odds ratio: 2.87; 95% confidence interval: 1.18-7.02), a rapid plasma regain titer >1: 128 (2.83; 1.11-7.26), and male sex (2.46; 1.06-5.70). Use of any highly active antiretroviral therapy before syphilis infection reduced the odds of neurosyphilis by 65% (0.35; 0.14-0.91). Sixty-three percent of cases presented with early neurosyphilis and the median time to neurosyphilis diagnosis was 9 months. Symptomatic patients had more cerebrospinal fluid abnormalities on initial lumbar puncture than asymptomatic patients (P = 0.01). Follow-up lumbar puncture within 12 months revealed that only 38% had resolution of all cerebrospinal fluid abnormalities. At 1 year, 38% had persistence of their major symptom despite adequate treatment for neurosyphilis. Twelve of 41 (29%) patients were retreated for syphilis.
Conclusion: Early neurosyphilis was common in this cohort. Highly active antiretroviral therapy to reverse immunosuppression may help mitigate neurological complications of syphilis.
Figures
References
-
- Musher DM. Syphilis, neurosyphilis, penicillin, and AIDS. J Infect Dis. 1991;163:1201–1206. - PubMed
-
- Berry CD, Hooton TM, Collier AC, Lukehart SA. Neurologic relapse after benzathine penicillin therapy for secondary syphilis in a patient with HIV infection. N Engl J Med. 1987;316:1587–1589. - PubMed
-
- Johns DR, Tierney M, Felsenstein D. Alteration in the natural history of neurosyphilis by concurrent infection with the human immunodeficiency virus. N Engl J Med. 1987;316:1569–1572. - PubMed
-
- Katz DA, Berger JR. Neurosyphilis in acquired immunodeficiency syndrome. Arch Neurol. 1989;46:895–898. - PubMed
-
- Berger JR. Neurosyphilis in human immunodeficiency virus type 1-seropositive individuals. A prospective study. Arch Neurol. 1991;48:700–702. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
