

Case Reports
The Gordon Wilson Lecture: work hours, sleep and patient safety in residency training
Affiliations
- PMID: 18528472
- PMCID: PMC1500922
Item in Clipboard
Case Reports
The Gordon Wilson Lecture: work hours, sleep and patient safety in residency training
Trans Am Clin Climatol Assoc.
2006.
No abstract available
Figures
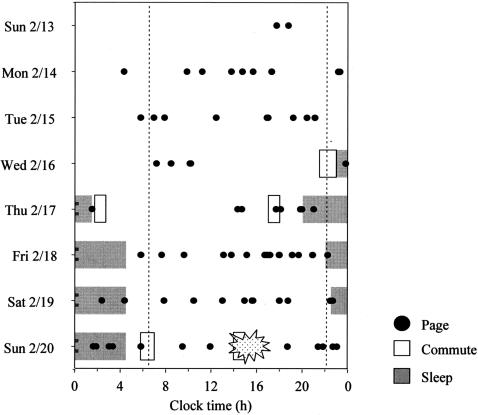
The sleep-wake times, commute times and pages (from the Brigham and Women’s Hospital paging records) of a PGY-5 Anesthesia Fellow leading up to motor vehicle crash.
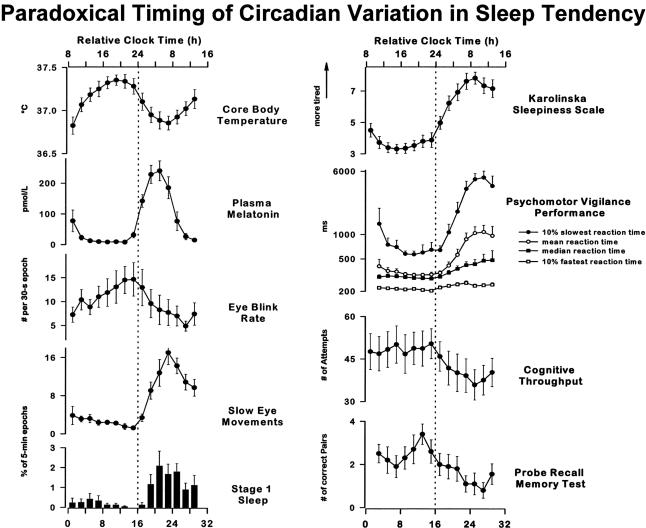
Laft-hand column: Time courses of core body temperature, endogenous plasma melatonin, mean eye blink rate per 30-s epoch during Karolinska drowsiness test (KDT), incidence of slow eye movements (SEMs, percentage of 30-s epochs containing at least 1 SEM/5-min interval), and incidence of stage 1 sleep (% of 30-s epochs containing at least 15 s of stage 1 sleep per 5-min interval) are shown, averaged across 10 subjects+ SE. Right-hand column: Time course of subjective sleepiness as assessed on Karolinska sleepiness scale (KSS; highest possible score = 9, lowest possible score = 1), psychomotor vigilance performance [mean, median, 10% slowest and fastest reaction times in ms (logarithmic scale)], cognitive performance (numbers of attempt in 4-min 2-digit addition task), and memory performance (number of correct word pairs in probed recall memory task) are shown averaged across 10 subjects+ SE. All data were binned in 2-h intervals and expressed with respect to elapsed time since scheduled waketime. Vertical reference line indicates subject’s habitual bedtime. Reprinted with permission from Cajochen et al (20). Copyright 1999 American Physiological Society.
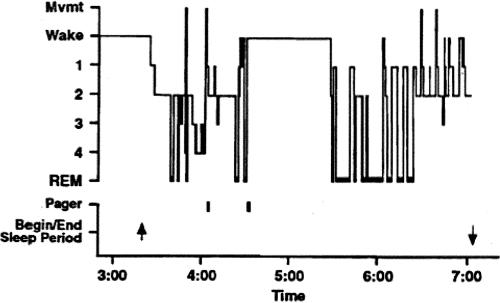
Polysomnographic recording of sleep in an intern on call. The figure depicts the hypnogram and the effects of two pages during the night in an intern from the group not covered by a night float. “Pager” indicates an electronically recorded page was issued to the intern’s beeper at the time indicated on the X-axis. “Begin/End sleep period” indicate the times recorded by the intern for these events in the diary. This record demonstrates the variable impact of pages during sleep. The first page, from one of the nursing stations, occurred at approximately 4.08 am. The page occurred while the intern was in stage 4 and produced only a brief movement without unambiguous awakening. Approximately 28 minutes later, the same nursing station paged again, this time awakening the intern from REM sleep. The intern subsequently remained awake for almost an hour despite no additional pager activity. Reprinted with permission from Richardson et al (26). Copyright 1996 Associated Professional Sleep Societies, LLC.
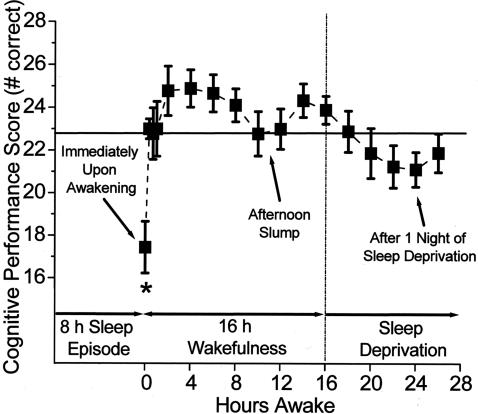
Impact of sleep inertia on cognitive performance upon awakening compared with 24 hours without sleep. Reprinted with permission from Wertz et al. (83). Copyright 2006 American Medical Association.
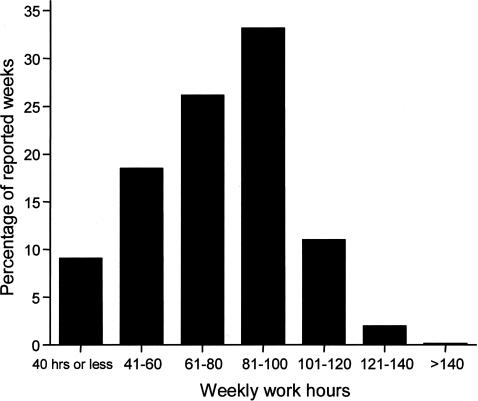
A total of 17,003 person-months of data were collected from a nationwide sample during 2002–2003. The distribution of the percentages of reported weeks with a given range of work hours is shown in this chart. Reprinted with permission from Barger et al (85). Copyright 2005 Massachusetts Medical Society.
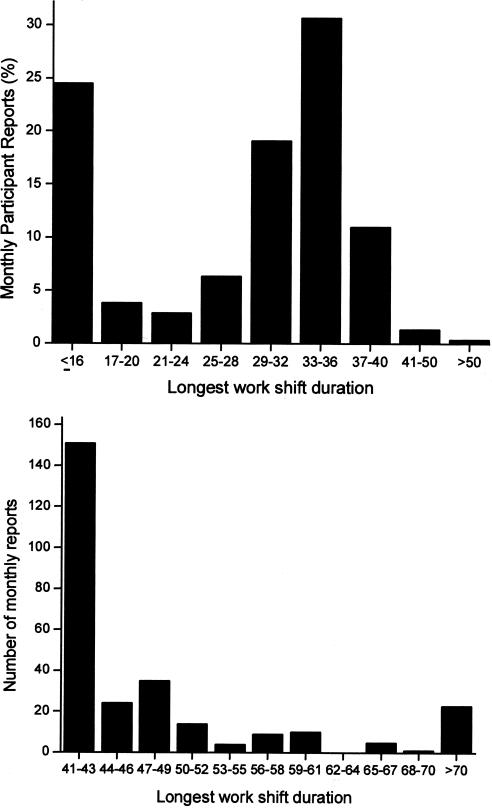
The longest shifts reported by participants are shown in the chart at the top. The chart at the bottom shows the number of surveys in which participants reported shifts that exceeded 40 hours. Reprinted with permission from Barger et al (85). Copyright 2005 Massachusetts Medical Society.
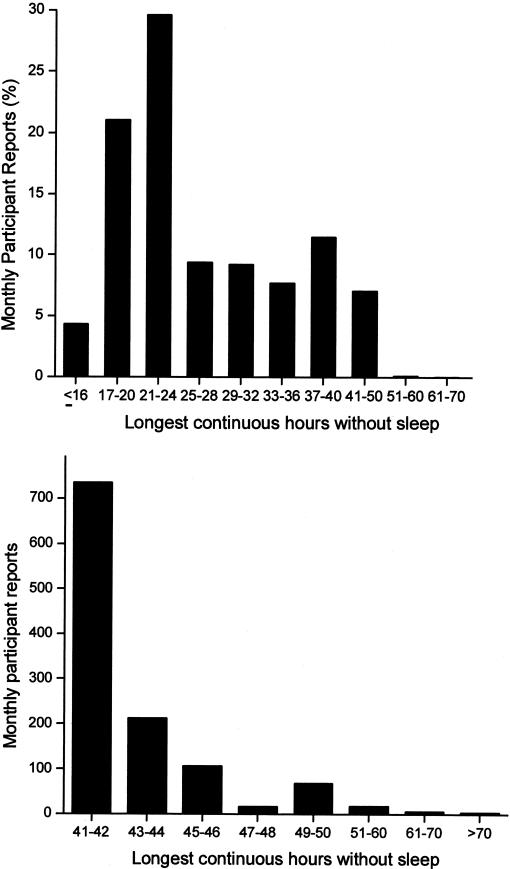
The greatest number of hours without sleep as a percentage of monthly reports is shown in the chart at the top. The chart at the bottom shows the number of surveys in which participants reported more than 40 continuous hours without sleep. Reprinted with permission from Barger et al (85). Copyright 2005 Massachusetts Medical Society.
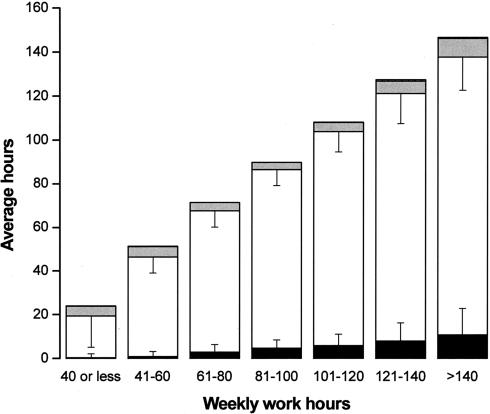
This chart shows the average number of hours that interns spent asleep in the hospital, awake in the hospital, studying or working in relation to their program but outside the hospital, and working outside of the program. T bars indicate standard deviations. Interns reported spending an average of 193.4+ 88.8 of their waking hours in the hospital each month participating in direct patient care (e.g., examining patients; writing progress notes; interpreting diagnostic tests, radiographic studies, and pathological specimens; and consulting with other physicians), 43.3+ 47.0 hours in duties not directly related to patient care (e.g., completing other paperwork and scheduling tests), 23.5+ 20.1 hours in structured learning sessions (including classes, laboratories, and grand rounds), and 7.3+ 16.4 hours teaching students or house staff. Reprinted with permission from Barger et al (85). Copyright 2005 Massachusetts Medical Society.
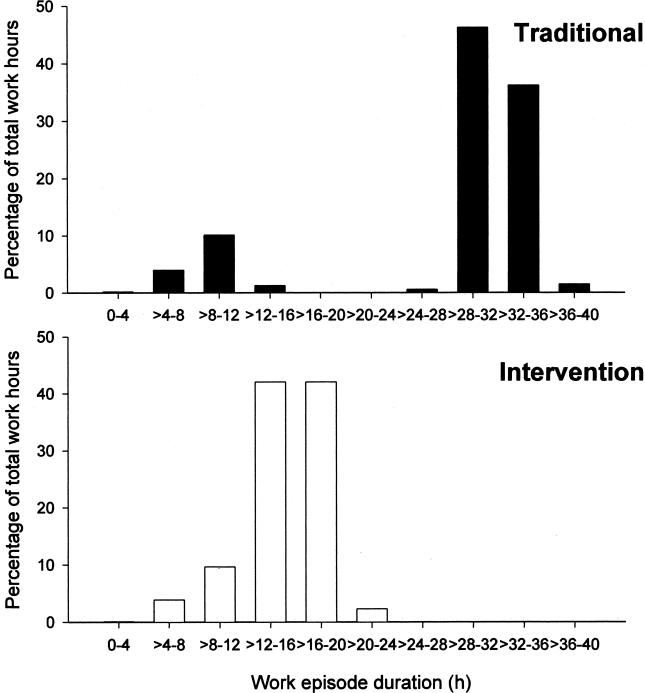
Proportion of total work hours plotted against the duration of the shift during the Traditional Schedule (top chart) and the Intervention Schedule (bottom chart). Reprinted with permission from Lockley et al (1). Copyright 2004 Massachusetts Medical Society.
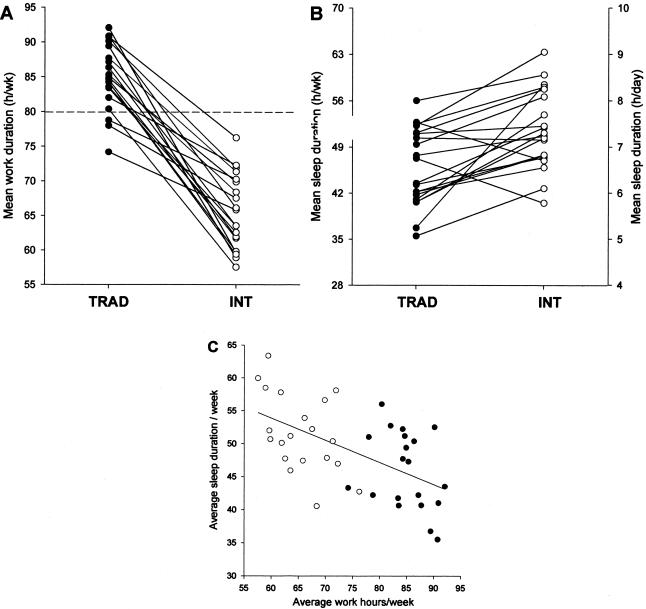
Subjective mean hours of work per week (top left), duration of sleep (top right), and the relationship between the duration of work and the duration of sleep (bottom chart) for 20 interns during the Traditional schedule and the Intervention schedule (open symbols). Reprinted with permission from Lockley et al (1). Copyright 2004 Massachusetts Medical Society.

Mean (+SE) number of attentional failures among the 20 interns as a group and individually while working overnight (11 pm to 7 am) during the Traditional schedule (filled bar) and the Intervention schedule (open bar). Reprinted with permission from Lockley et al (1). Copyright 2004 Massachusetts Medical Society.
References
-
- Lockley SW, Cronin JW, Evans EE, et al. fect of reducing interns’ weekly work hours on sleep and attentional failures. N Engl J Med. 2004;351:1829–1837. - PubMed
-
- Jewett ME. Models of circadian and homeostatic regulation of human performance and alertness. Harvard University. 1997
-
- Jewett ME, Borbély AA, Czeisler CA. oceedings of the workshop on biomathematical models of circadian rhythmicity, sleep regulations, and neurobehavioral function in humans. J Biol Rhythms. 1999;14:429–630. - PubMed
-
- Johnson MP, Duffy JF, Dijk DJ, Ronda JM, Dyal CM, Czeisler CA. hort-term memory, alertness and performance: A reappraisal of their relationship to body temperature. J Sleep Res. 1992;1:24–29. - PubMed
-
- Czeisler CA, Khalsa SBS. The human circadian timing system and sleep-wake regulation. In: Kryger MH, Roth T, Dement WC, editors. Principles and Practice of Sleep Medicine. Philadelphia: W.B. Saunders Company; 2000. pp. 353–374.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources