

Clinical and radiographic spectrum of pathologically confirmed tumefactive multiple sclerosis
- PMID: 18535080
- PMCID: PMC2442427
- DOI: 10.1093/brain/awn098
Clinical and radiographic spectrum of pathologically confirmed tumefactive multiple sclerosis
Abstract
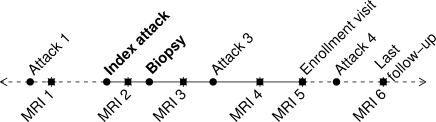
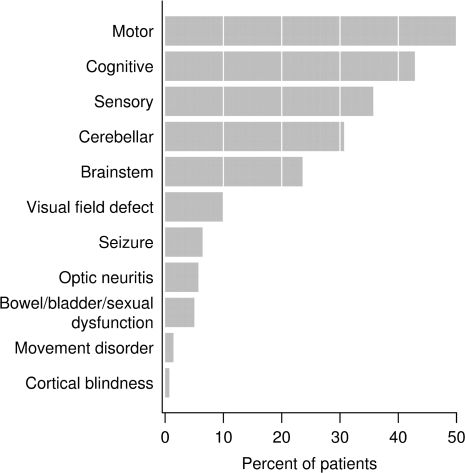
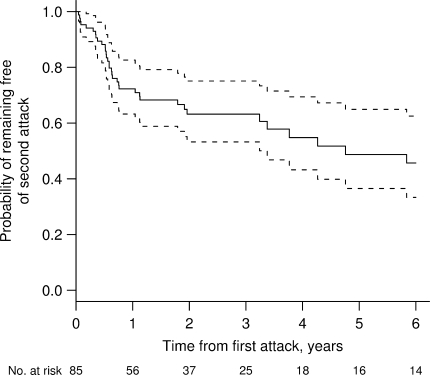
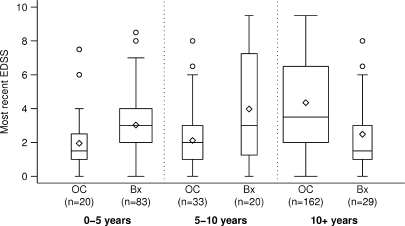
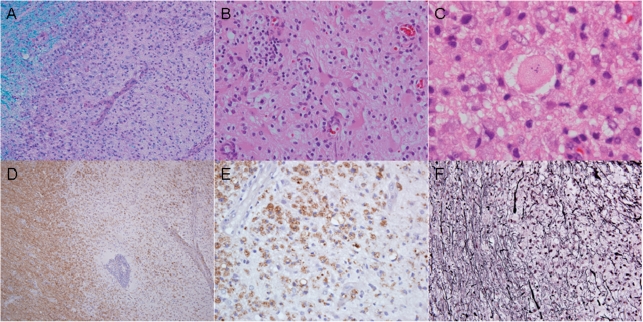
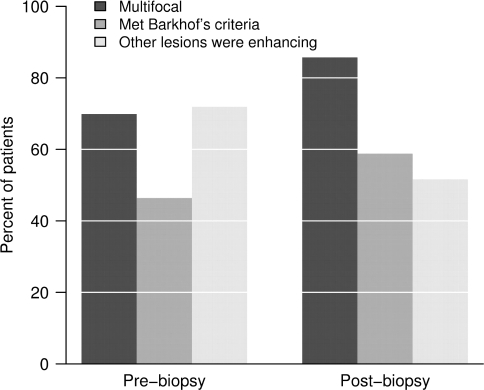
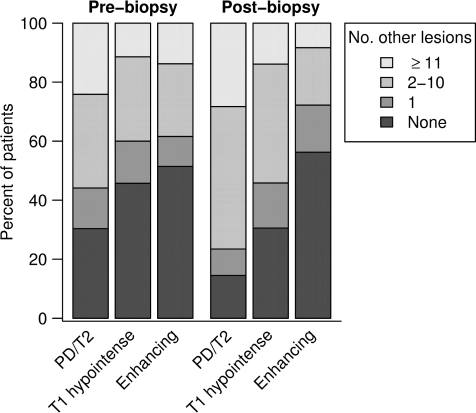
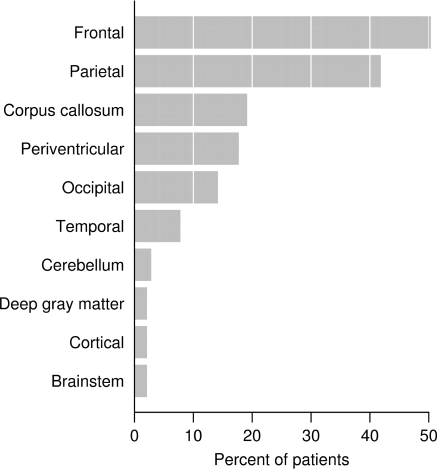
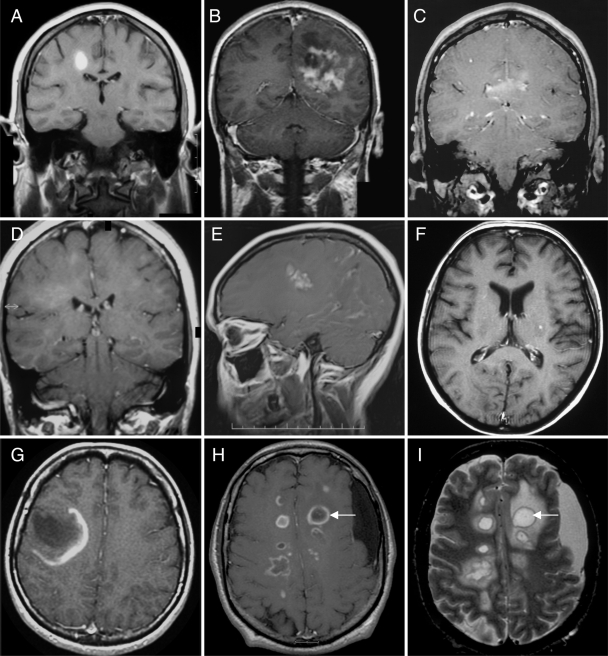
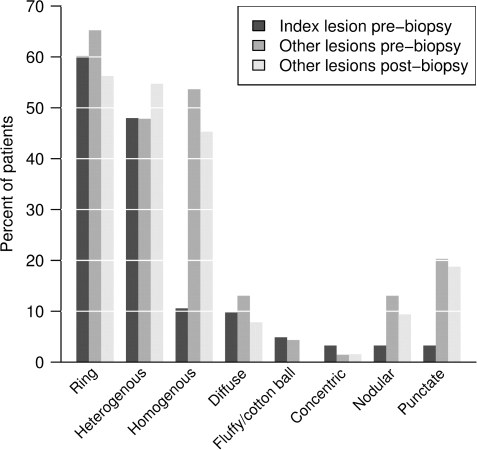
Atypical imaging features of multiple sclerosis lesions include size >2 cm, mass effect, oedema and/or ring enhancement. This constellation is often referred to as 'tumefactive multiple sclerosis'. Previous series emphasize their unifocal and clinically isolated nature, however, evolution of these lesions is not well defined. Biopsy may be required for diagnosis. We describe clinical and radiographic features in 168 patients with biopsy confirmed CNS inflammatory demyelinating disease (IDD). Lesions were analysed on pre- and post-biopsy magnetic resonance imaging (MRI) for location, size, mass effect/oedema, enhancement, multifocality and fulfilment of Barkhof criteria. Clinical data were correlated to MRI. Female to male ratio was 1.2 : 1, median age at onset, 37 years, duration between symptom onset and biopsy, 7.1 weeks and total disease duration, 3.9 years. Clinical course prior to biopsy was a first neurological event in 61%, relapsing-remitting in 29% and progressive in 4%. Presentations were typically polysymptomatic, with motor, cognitive and sensory symptoms predominating. Aphasia, agnosia, seizures and visual field defects were observed. At follow-up, 70% developed definite multiple sclerosis, and 14% had an isolated demyelinating syndrome. Median time to second attack was 4.8 years, and median EDSS at follow-up was 3.0. Multiple lesions were present in 70% on pre-biopsy MRI, and in 83% by last MRI, with Barkhof criteria fulfilled in 46% prior to biopsy and 55% by follow-up. Only 17% of cases remained unifocal. Median largest lesion size on T2-weighted images was 4 cm (range 0.5-12), with a discernible size of 2.1 cm (range 0.5-7.5). Biopsied lesions demonstrated mass effect in 45% and oedema in 77%. A strong association was found between lesion size, and presence of mass effect and/or oedema (P < 0.001). Ring enhancement was frequent. Most tumefactive features did not correlate with gender, course or diagnosis. Although lesion size >5 cm was associated with a slightly higher EDSS at last follow-up, long-term prognosis in patients with disease duration >10 years was better (EDSS 1.5) compared with a population-based multiple sclerosis cohort matched for disease duration (EDSS 3.5; P < 0.001). Given the retrospective nature of the study, the precise reason for biopsy could not always be determined. This study underscores the diagnostically challenging nature of CNS IDDs that present with atypical clinical or radiographic features. Most have multifocal disease at onset, and develop RRMS by follow-up. Although increased awareness of this broad spectrum may obviate need for biopsy in many circumstances, an important role for diagnostic brain biopsy may be required in some cases.
Figures
References
-
- Al-Bunyan MA. Tumor-like presentation of multiple sclerosis. Saudi Med J. 2000;21:393–5. - PubMed
-
- Annesley-Williams D, Farrell MA, Staunton H, Brett FM. Acute demyelination, neuropathological diagnosis, and clinical evolution. J Neuropathol Exp Neurol. 2000;59:477–89. - PubMed
-
- Annunziata P, Giorgio A, De Santi L, Zipoli V, Portaccio E, Amato MP, et al. Absence of cerebrospinal fluid oligoclonal bands is associated with delayed disability progression in relapsing-remitting MS patients treated with interferon-B. J Neurol Sci. 2006;244:97–102. - PubMed
-
- Atlas SW, Grossman RI, Gomori JM, Hackney DB, Goldberg HI, Zimmerman RA, et al. Hemorrhagic intracranial malignant neoplasms: spin-echo MR imaging. Radiology. 1987;164:71–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
