

Torcetrapib-induced blood pressure elevation is independent of CETP inhibition and is accompanied by increased circulating levels of aldosterone
- PMID: 18536749
- PMCID: PMC2440088
- DOI: 10.1038/bjp.2008.229
Torcetrapib-induced blood pressure elevation is independent of CETP inhibition and is accompanied by increased circulating levels of aldosterone
Abstract
Background and purpose: Inhibition of cholesteryl ester transfer protein (CETP) with torcetrapib in humans increases plasma high density lipoprotein (HDL) cholesterol levels but is associated with increased blood pressure. In a phase 3 clinical study, evaluating the effects of torcetrapib in atherosclerosis, there was an excess of deaths and adverse cardiovascular events in patients taking torcetrapib. The studies reported herein sought to evaluate off-target effects of torcetrapib.
Experimental approach: Cardiovascular effects of the CETP inhibitors torcetrapib and anacetrapib were evaluated in animal models.
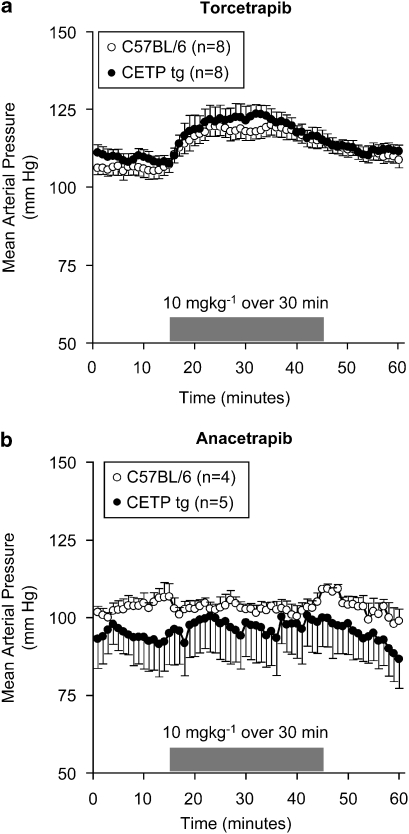
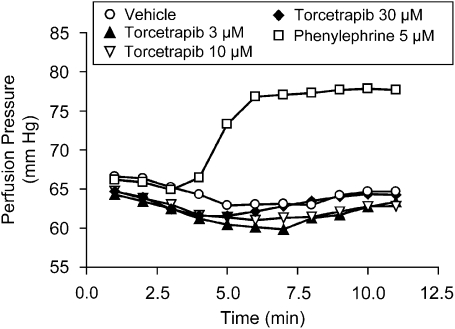
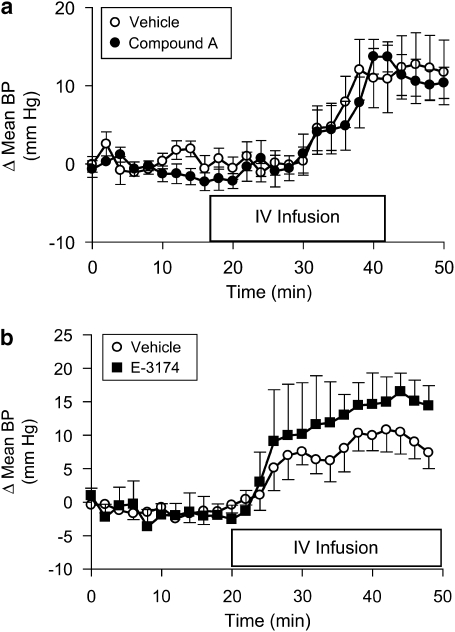
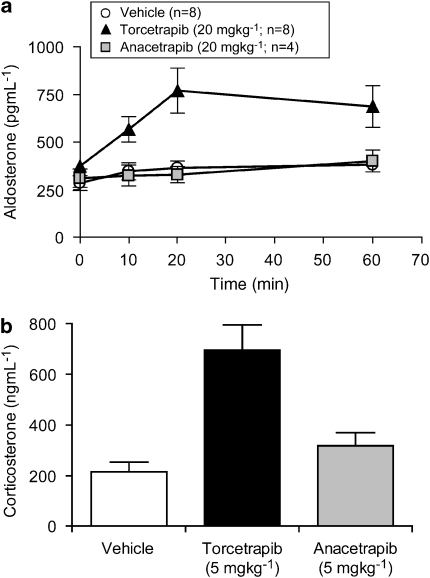
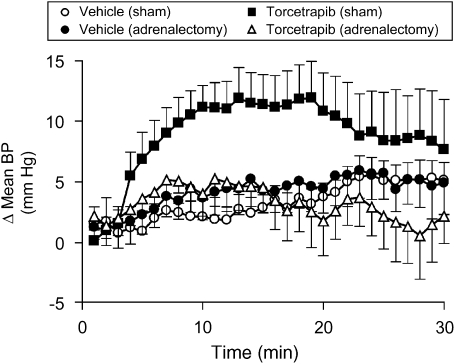
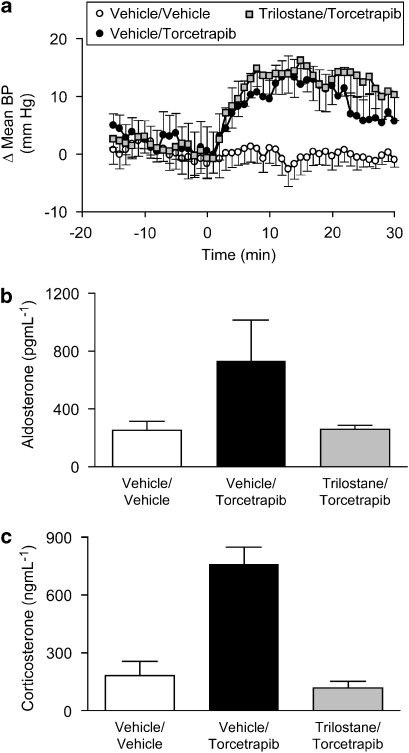
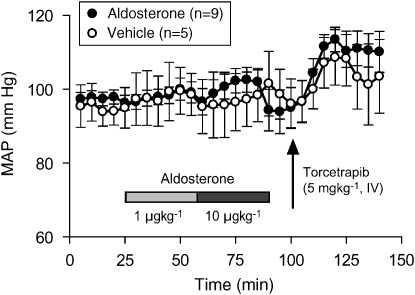
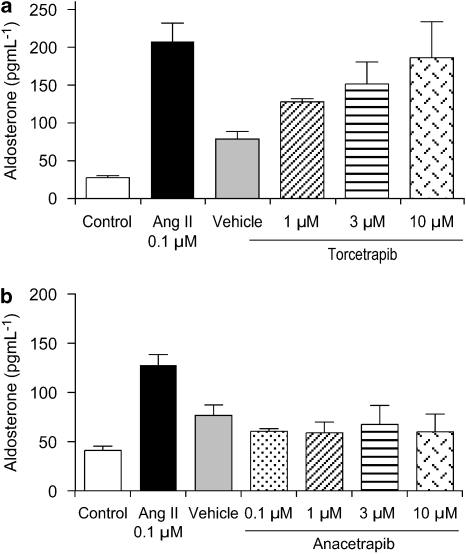
Key results: Torcetrapib evoked an acute increase in blood pressure in all species evaluated whereas no increase was observed with anacetrapib. The pressor effect of torcetrapib was not diminished in the presence of adrenoceptor, angiotensin II or endothelin receptor antagonists. Torcetrapib did not have a contractile effect on vascular smooth muscle suggesting its effects in vivo are via the release of a secondary mediator. Treatment with torcetrapib was associated with an increase in plasma levels of aldosterone and corticosterone and, in vitro, was shown to release aldosterone from adrenocortical cells. Increased adrenal steroid levels were not observed with anacetrapib. Inhibition of adrenal steroid synthesis did not inhibit the pressor response to torcetrapib whereas adrenalectomy prevented the ability of torcetrapib to increase blood pressure in rats.
Conclusions and implications: Torcetrapib evoked an acute increase in blood pressure and an acute increase in plasma adrenal steroids. The acute pressor response to torcetrapib was not mediated by adrenal steroids but was dependent on intact adrenal glands.
Figures
Comment in
-
The failure of torcetrapib: what have we learned?Br J Pharmacol. 2008 Aug;154(7):1379-81. doi: 10.1038/bjp.2008.248. Epub 2008 Jun 9. Br J Pharmacol. 2008. PMID: 18536741 Free PMC article.
References
-
- Assmann G, Schulte H. Relation of high density lipoprotein cholesterol and triglycerides to incidence of atherosclerotic coronary artery disease (the PROCAM experience) Am J Cardiol. 1992;70:733–737. - PubMed
-
- Barter PJ, Brewer HB, Jr, Chapman MJ, Hennekens CH, Rader DJ, Tall AR. Cholesteryl ester transfer protein: a novel target for raising HDL and inhibiting atherosclerosis. Arterioscler Thromb Vasc Biol. 2003;23:160–167. - PubMed
-
- Barter PJ, Caulfield M, Eriksson M, Grundy SM, Kastelein JJP, Komajda M, et al. Effects of torcetrapib in patients at high risk for coronary events. N Engl J Med. 2007;357:2109–2122. - PubMed
-
- Brousseau ME, Schaefer EJ, Wolfe ML, Bloedon LT, Digenio AG, Clark RW, et al. Effects of an inhibitor of cholesteryl ester transfer protein on HDL cholesterol. N Engl J Med. 2004;350:1505–1515. - PubMed
-
- Clark RW, Sutfin TA, Ruggeri RB, Willauer AT, Sugarman ED, Magnus-Aryitey G, et al. Raising high-density lipoprotein in humans through inhibition of cholesteryl ester transfer protein: an initial multidose study of torcetrapib. Arterioscler Thromb Vasc Biol. 2004;24:490–497. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
