

Diagnosing displaced four-part fractures of the proximal humerus: a review of observer studies
- PMID: 18536918
- PMCID: PMC2899076
- DOI: 10.1007/s00264-008-0591-2
Diagnosing displaced four-part fractures of the proximal humerus: a review of observer studies
Abstract
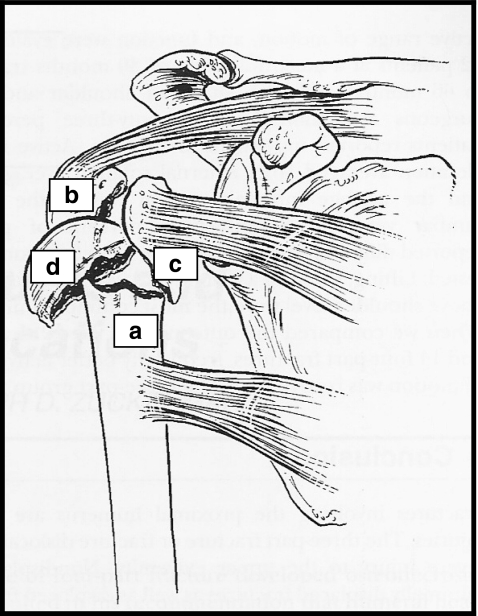
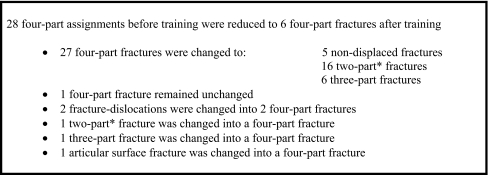
Displaced four-part fractures comprise 2-10 % of all proximal humeral fractures. The optimal treatment is unclear and randomised trials are needed. The conduct and interpretation of such trials is facilitated by a reproducible fracture classification. We aimed at quantifying observer agreement on the classification of displaced four-part fractures according to the Neer system. Published and unpublished data from five observer studies were reviewed. Observers agreed less on displaced four-part fractures than on the overall Neer classification. Mean kappa values for interobserver agreement ranged from 0.16 to 0.48. Specialists agreed slightly more than fellows and residents. Advanced imaging modalities (CT and 3D CT) seemed to contribute more to classification of displaced four-part patterns than in less complex fracture patterns. Low observer agreement may challenge the clinical approach to displaced four-part fractures and poses a problem for the interpretation and generalisation of results from future randomised trials.
Les fractures à quatre parts représentent 2 à 10% du total des fractures de l'extrémité supérieure de l'humérus. Le traitement optimal de ces fractures n'est pas évident. Une randomisation est nécessaire. De tels essais randomisés sont possibles si l'on dispose d'une classification fiable et reproductible de ces fractures. Les données publiées ou non publiées concernant 5 études ont été examinées. Notre but était également d'évaluer la classification en fonction de l'évolution. Pour les observateurs, sur l'ensemble de cette classification, les fracture à quatre parts étaient les plus difficiles à évaluer et la consolidation moins fiable. Les observations inter observateurs sont étalées de 0,16 à 0,48 sur le plan statistique (tests Kappa), l'avis des médecins spécialistes étant légèrement différent des « fellows » et des « résidents ». L'utilisation d'un scanner et notamment d'un scanner à trois dimensions a permis semble-t-il de mieux contribuer à la classification de ces fractures. Tout ceci intervient dans l'évaluation clinique de ces patients et pose le problème de l'interprétation, des résultats pour de futures études randomisées.
Figures


References
-
- Bengner U, Johnell O, Redlund-Johnell I. Changes in the incidence of fracture of the upper end of the humerus during a 30-year period. A study of 2125 fractures. Clin Orthop Relat Res. 1988;231:179–182. - PubMed
-
- Murray D, Zuckerman JD. Four-part fractures and fracture-dislocations. In: Zuckerman JD, Koval KJ, editors. Shoulder fractures. The practical guide to management. New York: Thieme; 2005. pp. 295–298.
-
- Lee EW, Flatow EL. Arthroplasty for proximal humerus fractures, nonunions, and malunions. In: Bigliani LU, Flatow EL, editors. Shoulder arthroplasty. New York: Springer; 2005. pp. 86–116.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
