

Preserving and evaluating hearts with ex vivo machine perfusion: an avenue to improve early graft performance and expand the donor pool
- PMID: 18539041
- PMCID: PMC2649718
- DOI: 10.1016/j.ejcts.2008.03.043
Preserving and evaluating hearts with ex vivo machine perfusion: an avenue to improve early graft performance and expand the donor pool
Abstract
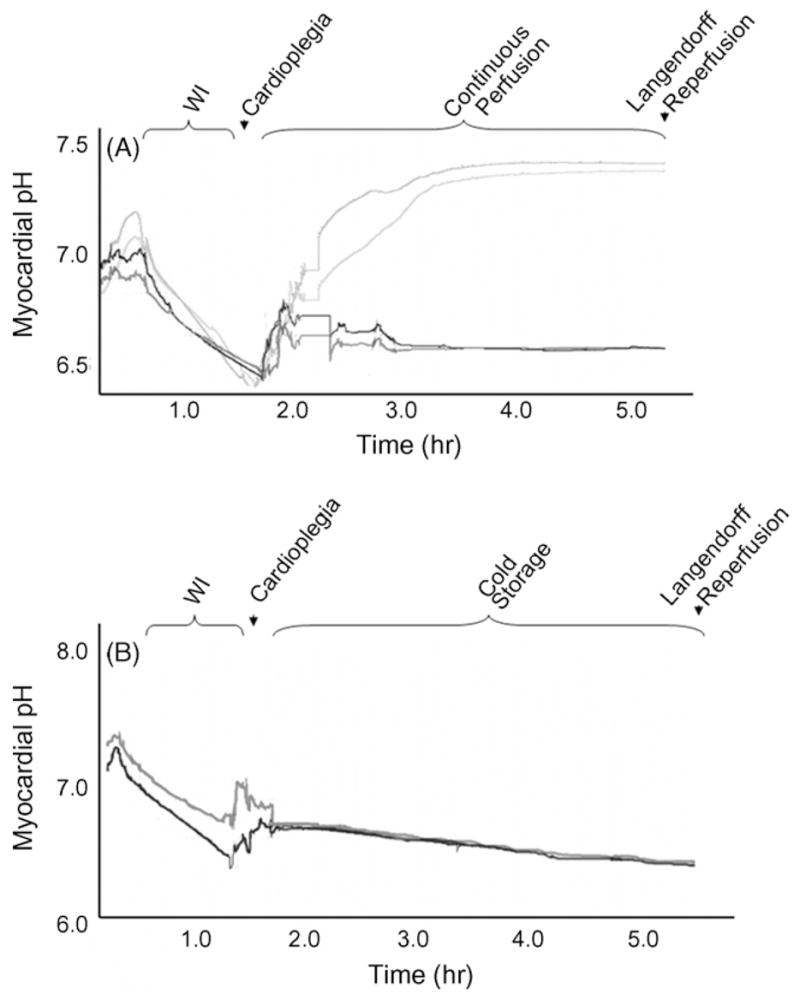
Cardiac transplantation remains the first choice for the surgical treatment of end stage heart failure. An inadequate supply of donor grafts that meet existing criteria has limited the application of this therapy to suitable candidates and increased interest in extended criteria donors. Although cold storage (CS) is a time-tested method for the preservation of hearts during the ex vivo transport interval, its disadvantages are highlighted in hearts from the extended criteria donor. In contrast, transport of high-risk hearts using hypothermic machine perfusion (MP) provides continuous support of aerobic metabolism and ongoing washout of metabolic byproducts. Perhaps more importantly, monitoring the organ's response to this intervention provides insight into the viability of a heart initially deemed as extended criteria. Obviously, ex vivo MP introduces challenges, such as ensuring homogeneous tissue perfusion and avoiding myocardial edema. Though numerous groups have experimented with this technology, the best perfusate and perfusion parameters needed to achieve optimal results remain unclear. In the present review, we outline the benefits of ex vivo MP with particular attention to how the challenges can be addressed in order to achieve the most consistent results in a large animal model of the ideal heart donor. We provide evidence that MP can be used to resuscitate and evaluate hearts from animal and human extended criteria donors, including the non-heart beating donor, which we feel is the most compelling argument for why this technology is likely to impact the donor pool.
Figures
References
-
- O’Connell JB, Bourge RC, Costanzo-Nordin MR, Driscoll DJ, Morgan JP, Rose EA, Uretsky BF. Cardiac transplantation: recipient selection, donor procurement, and medical follow-up. A statement for health professionals from the Committee on Cardiac Transplantation of the Council on Clinical Cardiology, American Heart Association. Circulation. 1992;86:1061–79. - PubMed
-
- Garrity ER, Moore J, Mulligan MS, Shearon TH, Zucker MJ, Murray S. Heart and lung transplantation in the United States, 1996–2005. Am J Transplant. 2007;7:1390–403. - PubMed
-
- Taylor DO, Edwards LB, Boucek MM, Trulock EP, Aurora P, Christie J, Dobbels F, Rahmel AO, Keck BM, Hertz MI. Registry of the International Society for Heart and Lung Transplantation: twenty-fourth official adult heart transplant report–2007. J Heart Lung Transplant. 2007;26:769–81. - PubMed
-
- Abouna GM. The use of marginal-suboptimal donor organs: a practical solution for organ shortage. Ann Transplant. 2004;9:62–6. - PubMed
-
- Buckberg GD, Brazier JR, Nelson RL, Goldstein SM, McConnell DH, Cooper N. Studies of the effects of hypothermia on regional myocardial blood flow and metabolism during cardiopulmonary bypass. I. The adequately perfused beating, fibrillating, and arrested heart. J Thorac Cardiovasc Surg. 1977;73:87–94. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
