

Review
doi: 10.1016/j.ccm.2008.03.010.
Pulmonary hypertension caused by sarcoidosis
Affiliations
- PMID: 18539244
- PMCID: PMC2593121
- DOI: 10.1016/j.ccm.2008.03.010
Item in Clipboard
Review
Pulmonary hypertension caused by sarcoidosis
Clin Chest Med.
2008 Sep.
Abstract
Pulmonary hypertension is an uncommon complication of sarcoidosis, but in severe pulmonary disease it occurs frequently. It is an important cause of cryptogenic dyspnea in sarcoidosis patients and can occur despite the absence of pulmonary fibrosis. The true prevalence is unknown. With the advent of specific therapies for pulmonary hypertension, there has been a resurgence of interest in the pathophysiology, diagnosis, and treatment of sarcoidosis-associated pulmonary hypertension. This article reviews the status of the current epidemiologic, pathophysiologic, and therapeutic knowledge regarding this entity.
Figures
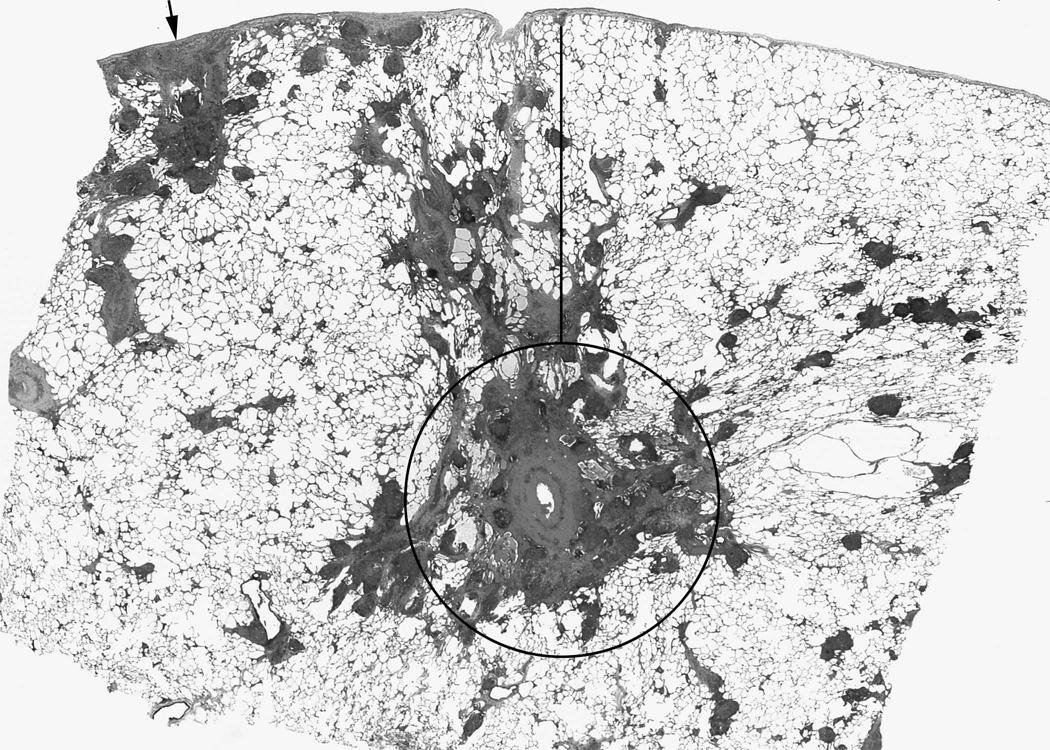
Sarcoidosis granulomas are found in a lymphatic distribution, including surrounding the bronchovascular bundle (circled area); the interlobular septae which also contain the pulmonary veins (adjacent to the line); and the subpleural area (arrow). Because of this anatomic orientation, granulomatous inflammation frequently encroaches on the vascular structures, even in the absence of overt fibrosis or vascular wall inflammation (Hematoxylin and eosin).
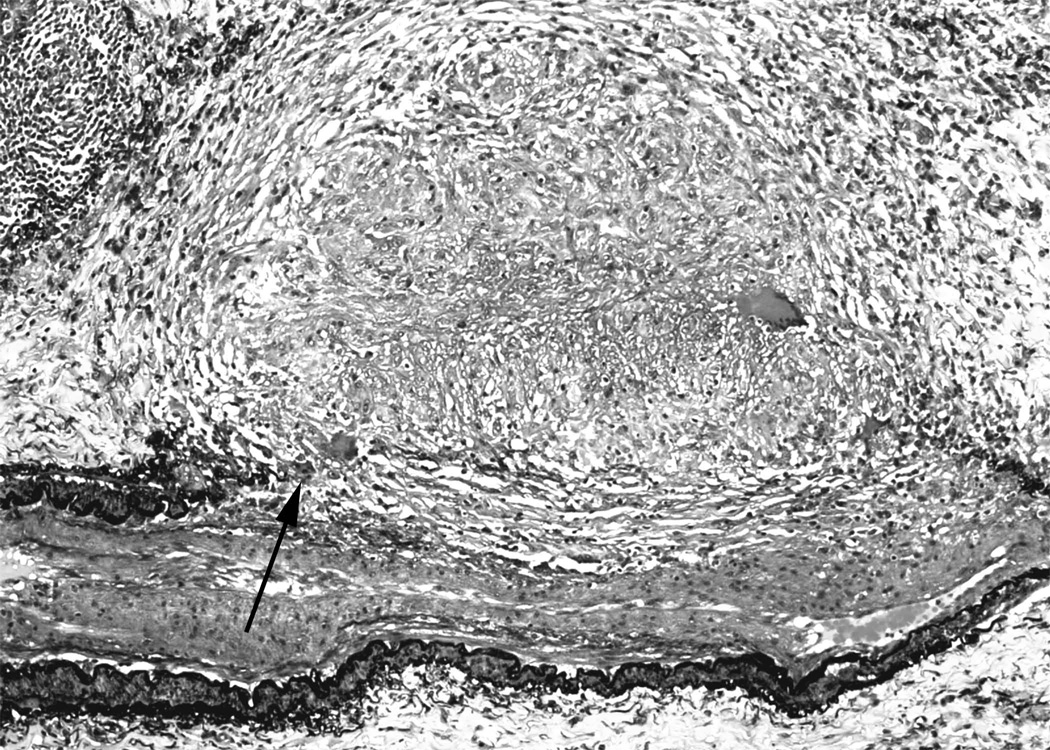
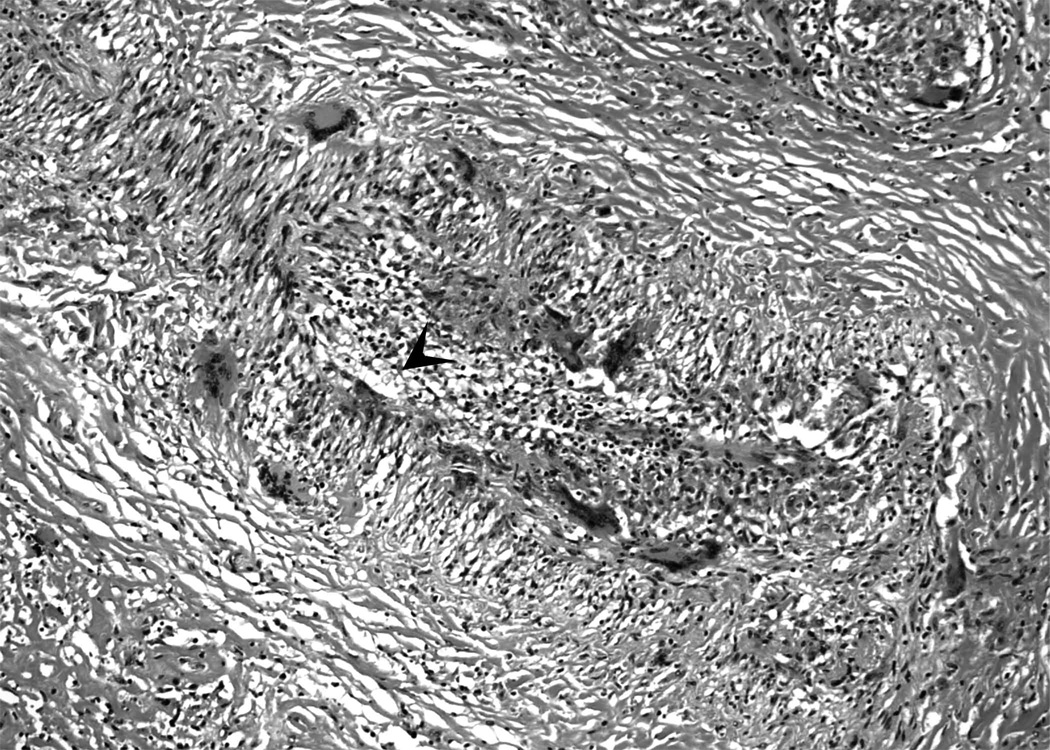
2a. Movat pentachrome stain showing granulomas obliterating the internal and external elastic laminae and smooth muscle (arrow) of medium size artery. There is secondary intimal fibroplasia seen in the center of the artery. (Movat pentachrome). 2b. In some cases, only giant cells and mononuclear cell infiltrates may be seen in sarcoidosis-associated arteritis. Arrowhead indicates the vascular lumen. Numerous giant cells may be seen in the vessel wall (Hematoxylin and eosin).
2a. Movat pentachrome stain showing granulomas obliterating the internal and external elastic laminae and smooth muscle (arrow) of medium size artery. There is secondary intimal fibroplasia seen in the center of the artery. (Movat pentachrome). 2b. In some cases, only giant cells and mononuclear cell infiltrates may be seen in sarcoidosis-associated arteritis. Arrowhead indicates the vascular lumen. Numerous giant cells may be seen in the vessel wall (Hematoxylin and eosin).
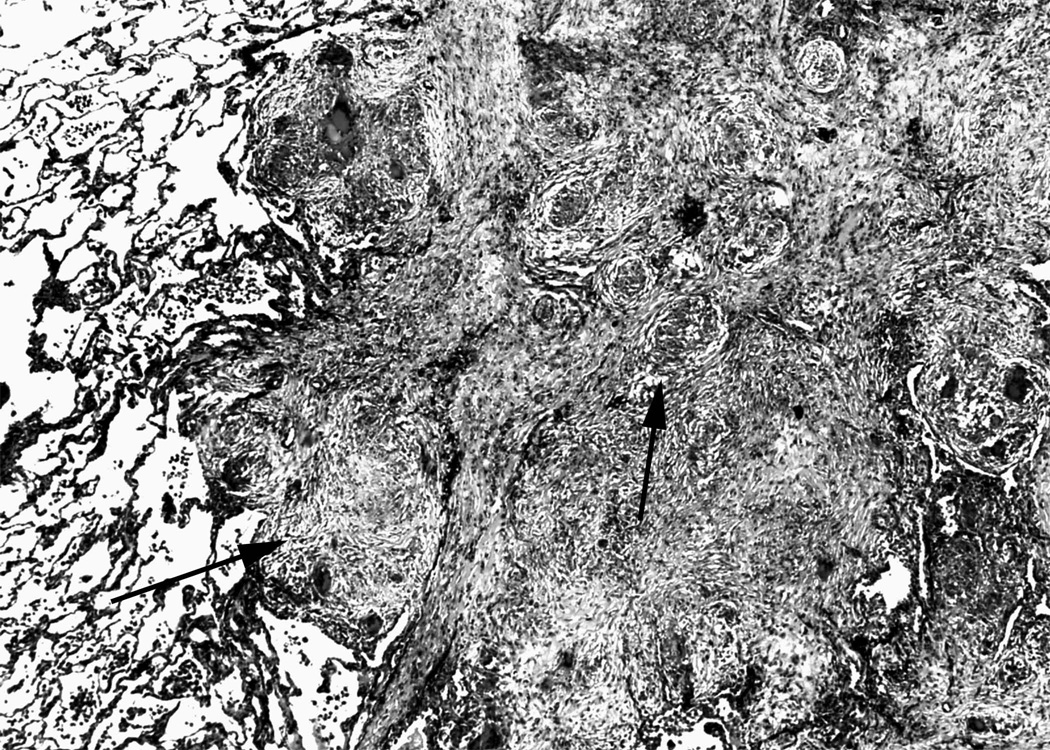
Movat pentachrome stain of an interlobular septum showing extensive fibrosis and obliteration of the venous structures by granulomas. Perivenular distribution of granulomas is typical in sarcoidosis. Arrows indicate compressive granulomas. (Movat pentachrome).
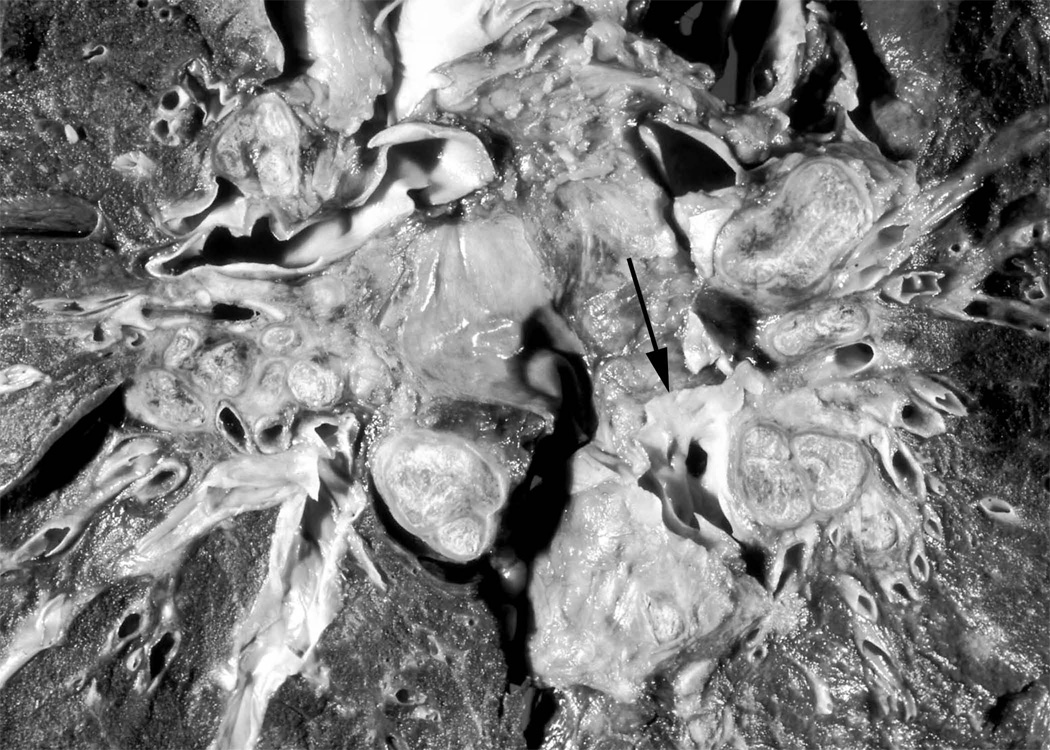
Coronal section of thorax of post-mortem specimen from a patient who died from end-stage SAPH. There is extensive hilar compression of the main pulmonary arteries. Arrow denotes the left lower lobe pulmonary artery, which is subtotally occluded by extrinsic compression of calcified lymph nodes that are present throughout the mediastinum. Image reproduced from Farver CF. Chapter 31: Sarcoidosis. In Dail and Hammar’s Pulmonary Pathology, 3rd edition. Editors, Tomashefski, Cagle, Farver, Fraire. Figure 18B. With kind permission of Springer Science and Business Media.
References
-
- Henderson LJ. Blood: a study in general physiology. London: Oxford University Press; 1928.
-
- Simonneau G, Galie N, Rubin LJ, et al. Clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2004;43:5S. - PubMed
-
- Rubin LJ. Diagnosis and management of pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest. 2004;126:7S. - PubMed
-
- Jing ZC, Xu XQ, Han ZY, et al. Registry and survival study in chinese patients with idiopathic and familial pulmonary arterial hypertension. Chest. 2007;132:373. - PubMed
-
- Humbert M, Sitbon O, Chaouat A, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006;173:1023. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
