

First-trimester maternal serum PP13 in the risk assessment for preeclampsia
- PMID: 18539259
- PMCID: PMC2784814
- DOI: 10.1016/j.ajog.2008.01.013
First-trimester maternal serum PP13 in the risk assessment for preeclampsia
Abstract
Objective: The objective of the study was to determine whether first-trimester maternal serum placental protein 13 (PP13) concentrations can be used in the risk assessment for preeclampsia.
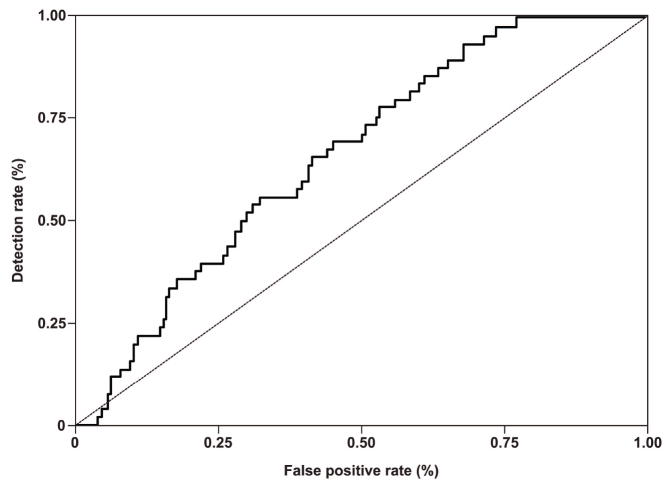
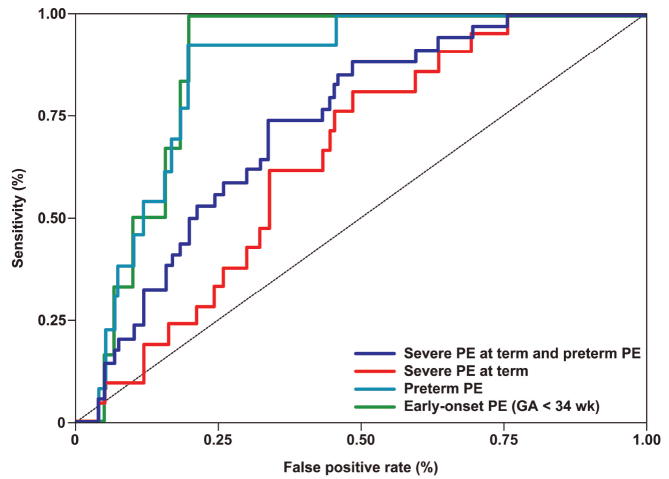
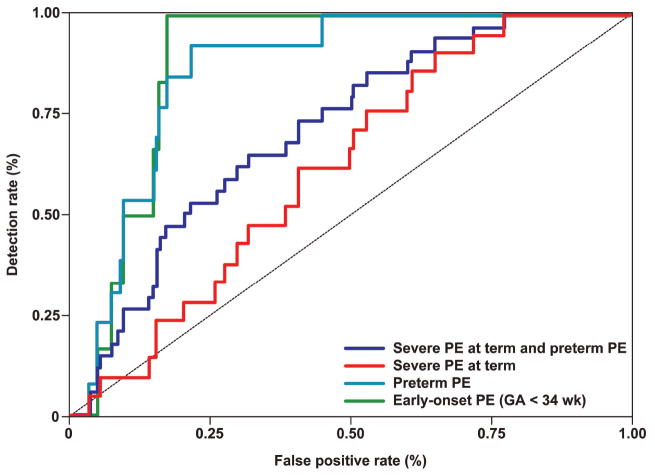
Study design: This case-control study included 50 patients with preeclampsia and 250 patients with normal pregnancies. Samples were collected between 8 and 13 weeks of gestation. Serum PP13 concentrations were measured by immunoassay and expressed as medians and multiples of the median (MoM) for gestational age. Sensitivity and specificity were derived from receiver-operating characteristic curve analysis.
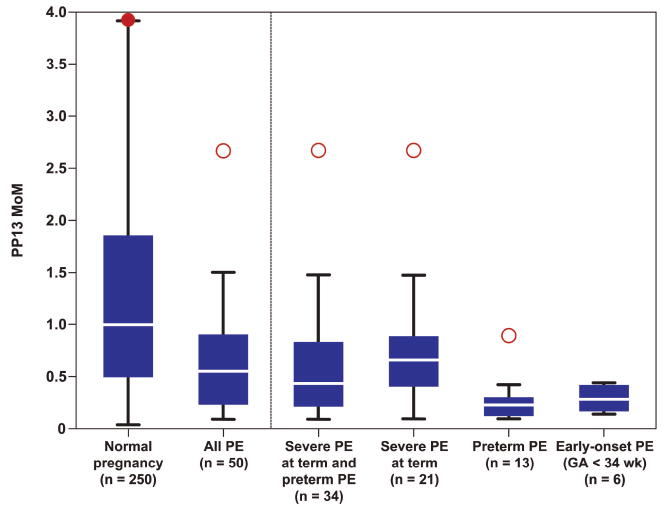
Results: (1) Serum PP13 concentration in the first trimester was significantly lower in patients who developed preterm and early-onset preeclampsia than in those with normal pregnancies; and (2) at 80% specificity, a cutoff of 0.39 MoM had a sensitivity of 100% for early-onset preeclampsia and 85% for preterm preeclampsia.
Conclusion: Maternal serum first-trimester PP13 appears to be a reasonable marker for risk assessment for preterm preeclampsia but a weak marker for severe preeclampsia at term, and ineffective for identifying mild preeclampsia at term.
Figures
References
-
- Sibai BM, Ewell M, Levine RJ, Klebanoff MA, Esterlitz J, Catalano PM, et al. Risk factors associated with preeclampsia in healthy nulliparous women. The Calcium for Preeclampsia Prevention (CPEP) Study Group. Am J Obstet Gynecol. 1997;177:1003–10. - PubMed
-
- Dekker GA, Sibai BM. Etiology and pathogenesis of preeclampsia: current concepts. Am J Obstet Gynecol. 1998;179:1359–75. - PubMed
-
- Confidential Enquiries in Maternal Deaths. Why Mothers Die 1997-1999. London: RCOG Press; 2002.
-
- Sibai BM, Caritis S, Hauth J. What we have learned about preeclampsia. Semin Perinatol. 2003;27:239–46. - PubMed
-
- National Institute for Clinical Excellence. Routine antenatal care for healthy pregnant woman. London: National Institute for Clinical Excellence; 2003.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
