

Associations between anisometropia, amblyopia, and reduced stereoacuity in a school-aged population with a high prevalence of astigmatism
- PMID: 18539935
- PMCID: PMC2573872
- DOI: 10.1167/iovs.08-1985
Associations between anisometropia, amblyopia, and reduced stereoacuity in a school-aged population with a high prevalence of astigmatism
Abstract
Purpose: To describe the relation between magnitude of anisometropia and interocular acuity difference (IAD), stereoacuity (SA), and the presence of amblyopia in school-aged members of a Native American tribe with a high prevalence of astigmatism.
Methods: Refractive error (cycloplegic autorefraction confirmed by retinoscopy), best corrected monocular visual acuity (VA; Early Treatment Diabetic Retinopathy Study logMAR charts), and best corrected SA (Randot Preschool Stereoacuity Test) were measured in 4- to 13-year-old Tohono O'odham children (N = 972). Anisometropia was calculated in clinical notation (spherical equivalent and cylinder) and in two forms of vector notation that take into account interocular differences in both axis and cylinder magnitude.
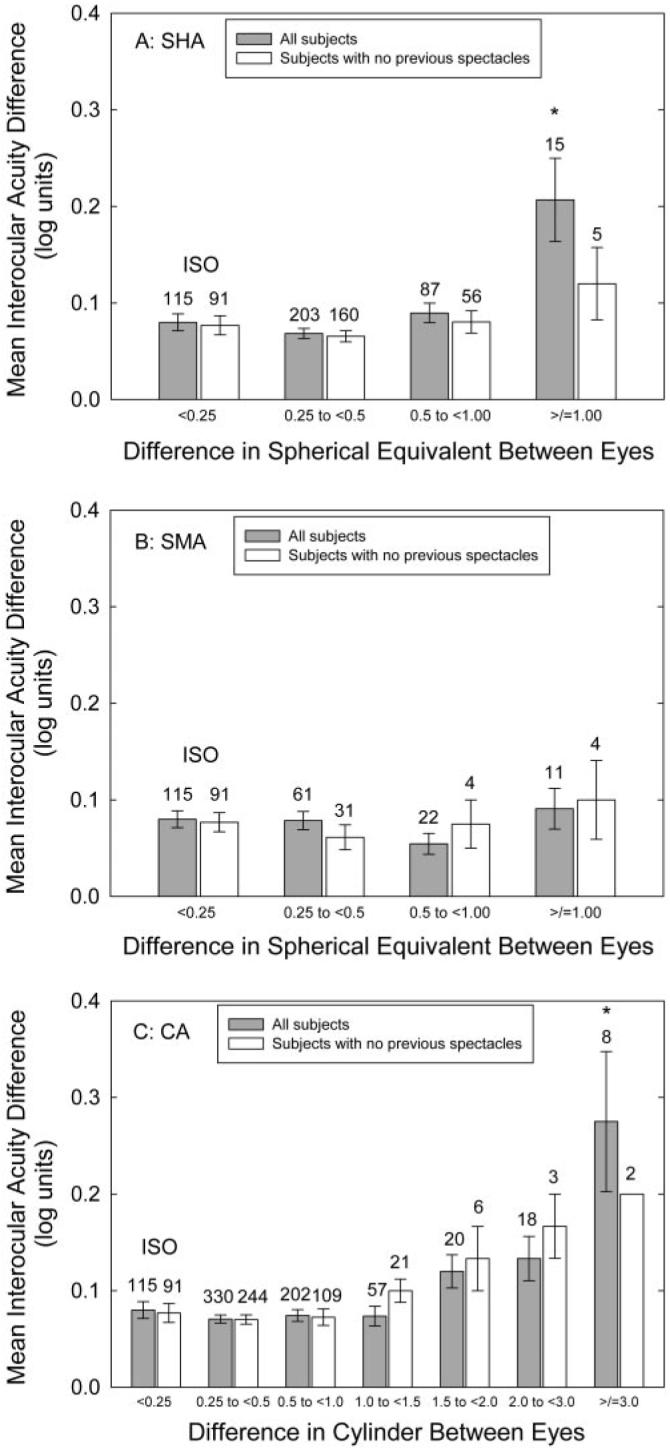
Results: Astigmatism >or= 1.00 D was present in one or both eyes of 415 children (42.7%). Significant increases in IAD and presence of amblyopia (IAD >or= 2 logMAR lines) occurred, with >or=1 D of hyperopic anisometropia and >or=2 to 3 D of cylinder anisometropia. Significant decreases in SA occurred with >or=0.5 D of hyperopic, myopic, or cylinder anisometropia. Results for vector notation depended on the analysis used, but also showed disruption of SA at lower values of anisometropia than were associated with increases in IAD and presence of amblyopia.
Conclusions: Best corrected IAD and presence of amblyopia are related to amount and type of refractive error difference (hyperopic, myopic, or cylindrical) between eyes. Disruption of best corrected random dot SA occurs with smaller interocular differences than those producing an increase in IAD, suggesting that the development of SA is particularly dependent on similarity of the refractive error between eyes.
Figures





Similar articles
-
Associations of anisometropia with unilateral amblyopia, interocular acuity difference, and stereoacuity in preschoolers.Ophthalmology. 2013 Mar;120(3):495-503. doi: 10.1016/j.ophtha.2012.08.014. Epub 2012 Nov 20. Ophthalmology. 2013. PMID: 23174398 Free PMC article.
-
Anisometropia prevalence in a highly astigmatic school-aged population.Optom Vis Sci. 2008 Jul;85(7):512-9. doi: 10.1097/OPX.0b013e31817c930b. Optom Vis Sci. 2008. PMID: 18594336 Free PMC article.
-
Optical treatment reduces amblyopia in astigmatic children who receive spectacles before kindergarten.Ophthalmology. 2009 May;116(5):1002-8. doi: 10.1016/j.ophtha.2008.11.013. Epub 2009 Feb 20. Ophthalmology. 2009. PMID: 19232733
-
Prevalence of anisometropia and its association with refractive error and amblyopia in preschool children.Br J Ophthalmol. 2013 Sep;97(9):1095-9. doi: 10.1136/bjophthalmol-2012-302637. Epub 2013 Apr 23. Br J Ophthalmol. 2013. PMID: 23613508 Review.
-
Observations on the relationship between anisometropia, amblyopia and strabismus.Vision Res. 2017 May;134:26-42. doi: 10.1016/j.visres.2017.03.004. Epub 2017 Apr 18. Vision Res. 2017. PMID: 28404522 Free PMC article. Review.
Cited by
-
Changes in anisometropia by age in children with hyperopia, myopia, and antimetropia.Sci Rep. 2023 Aug 22;13(1):13643. doi: 10.1038/s41598-023-40831-0. Sci Rep. 2023. PMID: 37608064 Free PMC article.
-
Refractive state in children with unilateral congenital nasolacrimal duct obstruction.J Ophthalmic Vis Res. 2012 Oct;7(4):310-5. J Ophthalmic Vis Res. 2012. PMID: 23503710 Free PMC article.
-
Stereoacuity in children with anisometropic amblyopia.J AAPOS. 2011 Oct;15(5):455-61. doi: 10.1016/j.jaapos.2011.06.007. J AAPOS. 2011. PMID: 22108357 Free PMC article.
-
Risk factors for amblyopia in the vision in preschoolers study.Ophthalmology. 2014 Mar;121(3):622-9.e1. doi: 10.1016/j.ophtha.2013.08.040. Epub 2013 Oct 18. Ophthalmology. 2014. PMID: 24140117 Free PMC article.
-
Threshold Values of Myopic Anisometropia Causing Loss of Stereopsis.J Ophthalmol. 2019 May 6;2019:2654170. doi: 10.1155/2019/2654170. eCollection 2019. J Ophthalmol. 2019. PMID: 31198605 Free PMC article.
References
-
- American Academy of Ophthalmology Pediatric Ophthalmology/Strabismus Panel . Preferred Practice Pattern Guidelines. Amblyopia. American Academy of Ophthalmology; San Francisco: 2007.
-
- American Optometric Association . Optometric Clinical Practice Guideline. Care of the Patient with Amblyopia. American Optometric Association; St. Louis: 2004.
-
- Donahue SP, Arnold RW, Ruben JB, AAPOS Vision Screening Committee Preschool vision screening: what should we be detecting and how should we report it?— uniform guidelines for reporting results of preschool vision screening studies. J AAPOS. 2003;7:314–316. - PubMed
-
- Gerali PS, Flom MC, Raab EL. Report of the Children's Vision Screening Task Force. National Society to Prevent Blindness; Schaumburg, IL: 1990.
-
- Caputo R, Frosini R, De Libero C, Campa L, Del Magro EF, Secci J. Factors influencing severity of and recovery from anisometropic amblyopia. Strabismus. 2007;15:209–214. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
