

Review
doi: 10.1161/CIRCULATIONAHA.107.760686.
Aortitis
Affiliations
- PMID: 18541754
- PMCID: PMC2759760
- DOI: 10.1161/CIRCULATIONAHA.107.760686
Item in Clipboard
Review
Aortitis
Circulation.
.
No abstract available
Figures
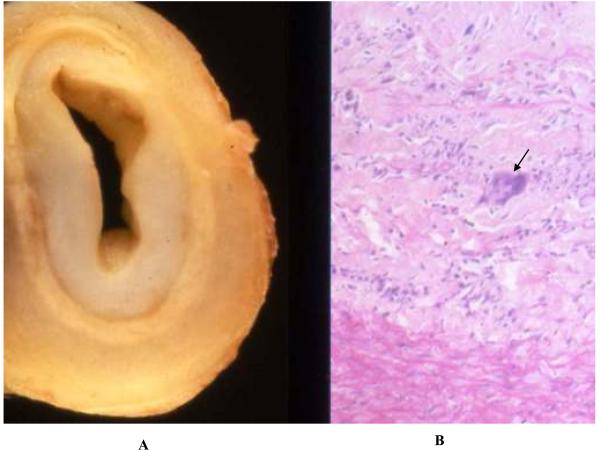
Pathologic findings in Takayasu arteritis. Shown are gross (Panel A) and histologic (Panel B) pathology of the innominate artery of a 27 year-old woman with Takayasu arteritis with arch vessel involvement. There is extensive intimal thickening with attenuation of the media and adventitial fibrosis (Panel A). Histology revealed degeneration of the media with a dense inflammatory infiltrate, including giant cells (arrow). (Image courtesy Dr. Richard N. Mitchell, Department of Pathology, Brigham and Women's Hospital).
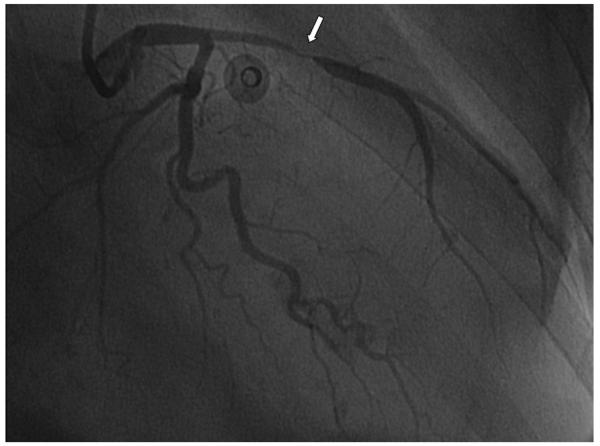
Coronary giant cell arteritis. This 75 year-old woman presented with non-ST segment elevation myocardial infarction and concomitant bilateral arm claudication. There is a tapering lesion in the left anterior descending artery (arrow), typical of GCA. (Reproduced from Jang, et al., with permission of the publisher).

Aortic occlusive disease in a patient with Takayasu arteritis and bilateral leg claudication. Shown are MRA images demonstrating severe, diffuse stenosis of the infrarenal abdominal aorta and common iliac arteries (Panels A and B). A prominent collateral vessel is noted (arrow). The patient underwent endovascular revascularization (Panel C, volume rendered CTA). (Image courtesy Drs. Gary Hoffman and Paul Schoenhagen, Cleveland Clinic Foundation).

Takayasu arteritis involving the coronary ostia. Shown are high-grade ostial stenoses of the left main coronary artery (Panel A) and right coronary artery (Panel B). Coronary involvement in association with Takayasu arteritis is generally ostial in location and due to aortitis at the aortic root. (Reproduced from Kang, et al., with permission of the publisher).
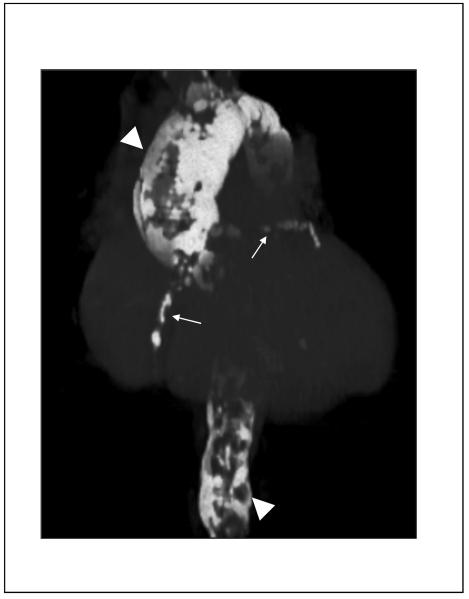
Computed tomogram of severe aortic and coronary calcification in a patient with a remote history of aortitis (“porcelain aorta”). Shown are volume-rendered CT images demonstrating severe calcification of the thoracic and abdominal aorta (arrowheads), as well as the coronary arteries (arrows). There is diffuse aneurysmal dilatation of the ascending thoracic aorta. (Image courtesy Dr. Paul Schoenhagen, Departments of Radiology and Cardiovascular Medicine, Cleveland Clinic Foundation).
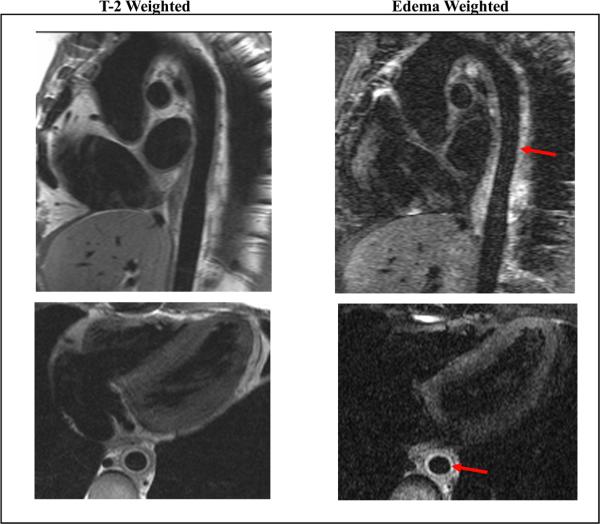
Magnetic resonance angiography in a patient with Takayasu arteritis and active aortitis. Shown are oblique sagittal (top row) and oblique axial (bottom row) images of the thoracic aorta with T-2 weighted black blood (left column) and edema-weighted imaging (right column). There is wall thickening of the descending thoracic aorta (best seen on axial images) with increased signal consistent with edema and inflammation (arrows). Periaortic inflammation and lymphadenopathy were also present. (Image courtesy Dr. Paul Schoenhagen, Departments of Radiology and Cardiovascular Medicine, Cleveland Clinic Foundation).
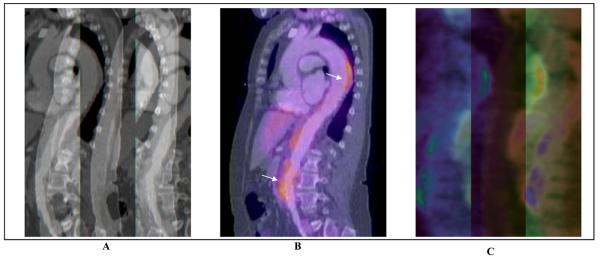
Combination of 18F-FDG PET and computed tomography for assessment of Takayasu arteritis. Shown are sagittal plane contrast-enhanced computed tomographic (CTA) images of the thoracic and abdominal aorta (Panel A), 18F-FDG PET – CTA overlay (Panel B), and 18F-FDG PET alone (Panel C). There are areas of FDG-uptake, consistent with inflammation, visualized in the descending thoracic and abdominal aorta. (Image courtesy Dr. Paul Schoenhagen, Departments of Radiology and Cardiovascular Medicine, Cleveland Clinic Foundation).
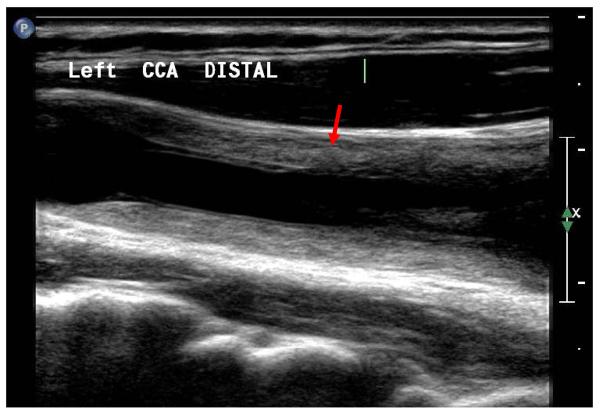
High resolution B-mode ultrasound of the common carotid artery a patient with active Takayasu arteritis. There is marked, diffuse, concentric thickening of the vessel wall with a heterogeneous appearance (arrow). The intimal-medial complex is markedly thickened. This finding has been termed the “macaroni sign”. No atherosclerotic plaque is visualized. Similar findings were present in the contralateral common carotid artery.
References
-
- Foote EA, Postier RG, Greenfield RA, Bronze MS. Infectious Aortitis. Curr Treat Options Cardiovasc Med. 2005;7:89–97. - PubMed
-
- Virmani R, Burke A. Nonatherosclerotic Diseases of the Aorta and Miscellaneous Disease of the Main Pulmonary Arteries and Large Veins. In: Silver M, Gotlieb A, Schoen F, editors. Cardiovascular Pathology. 3rd ed. Churchill Livingstone; Philadelphia: 2001. pp. 107–137.
-
- Gravanis MB. Giant cell arteritis and Takayasu aortitis: morphologic, pathogenetic and etiologic factors. Int J Cardiol. 2000;75(Suppl 1):S21–33. discussion S35-26. - PubMed
-
- Tavora F, Burke A. Review of isolated ascending aortitis: differential diagnosis, including syphilitic, Takayasu's and giant cell aortitis. Pathology. 2006;38:302–308. - PubMed
-
- Miller DV, Isotalo PA, Weyand CM, Edwards WD, Aubry MC, Tazelaar HD. Surgical pathology of noninfectious ascending aortitis: a study of 45 cases with emphasis on an isolated variant. Am J Surg Pathol. 2006;30:1150–1158. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
